9 Management of Findings Initially Detected at MRI
Hiroyuki Abe
Abstract
When abnormal findings are detected on breast MRI studies, the next step is to differentiate between probably benign lesions that do not need tissue sampling and suspicious lesions that need to be biopsied. The morphologic characteristics, kinetic assessment, patient’s risk factors, and the indications for MRI studies are taken into account in deciding whether tissue sampling is needed. Probably benign lesions can be followed in short term. For suspicious lesions, the next step is to determine a method of percutaneous biopsy. Although the mainstay of the biopsy method is MRI-guided biopsy, an ultrasound-guided biopsy or a stereotactic biopsy may be performed depending on the lesion type. Selection of a biopsy method must be made with careful observation of relevant images. Any suspicious lesions that are not visualized on any other imaging modalities than MRI should be biopsied under MRI guidance. The difficulty of MRI-guided biopsy is variable depending on the lesion location. Once a biopsy is performed, the physician who performed the biopsy should make a decision if the pathologic result is concordant or discordant with imaging findings. The decision making process in this series of studies requires considerable experience of the breast imaging.
9 Management of Findings Initially Detected at MRI
9.1 Introduction
Magnetic resonance imaging (MRI) is more sensitive in detecting breast lesions than conventional imaging by far, and is very useful for screening purposes. It is also true that MRI can be used for regional staging of a patient with known breast cancer, to look for satellites and determine the extent of a known malignancy. Due to its high sensitivity, however, MRI detects not only malignant lesions but also benign lesions. The challenge for MRI is to differentiate clearly between benign lesions that do not need tissue sampling and those suspicious lesions that need to be biopsied.
Table 9‑1 shows a summary of negative, benign, and probably benign lesions. In general, large mass lesions (>15 mm) with irregular shape, irregular or spiculated margins, heterogeneous or thick rim enhancement, and rapid enhancement tend to be malignant. Masses with homogeneous enhancement or dark internal septations and persistent kinetics tend to be benign. When evaluating any given lesion, it is important not only to evaluate the morphologic and kinetic characteristics, but also to take into account the patient’s risk factors, such as the presence of a genetic mutation or a strong family or personal history of breast cancer, before deciding whether tissue sampling is needed.
Table 9.1MRI features of normal, benign, and probable benign lesions
1. Normal
Edge enhancement
Nodular parenchymal enhancement
Lymph node
2. Benign lesions
Multiple similar-shaped and similar-sized lesions
Thin, regular rim enhancement
Nonenhancing lesions
Skin lesion
3. Probable benign lesions
Enhancing mass with dark internal septations
Slowly enhancing, circumscribed mass
Fat-containing lesion
Small linear NME (nonbranching)
Patient indications for MRI studies may also influence management. For example, an enhancing lesion initially seen on MRI tends to be malignant in patients who have metastatic axillary lymph nodes of unknown origin (CUP [carcinoma unknown primary] syndrome). Similarly, a finding in a patient referred with positive or close surgical margins following breast cancer surgery or with newly diagnosed breast cancer is more likely to require further investigation. A lesion identified in the same quadrant as that of a known cancer is likely to be a satellite lesion, and should be evaluated further. Availability of prior MRI examinations is very helpful for diagnosis, and when available, a search for interval change and new and developing lesions will aid in cancer detection.
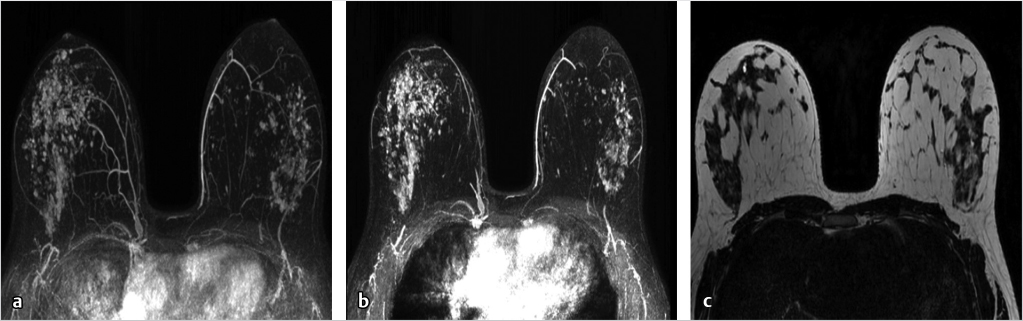
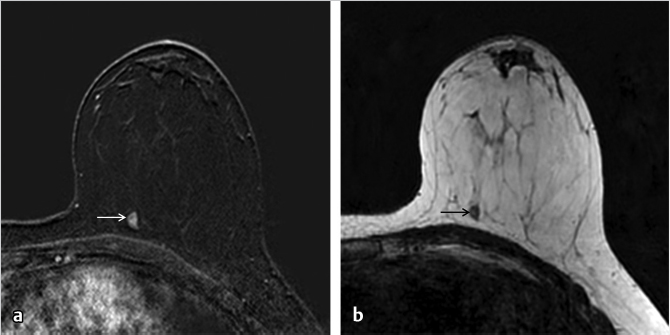
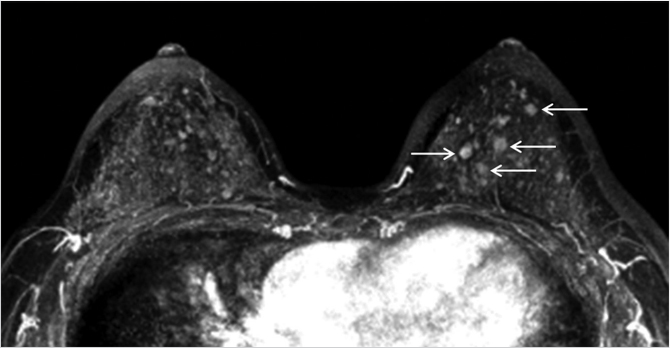
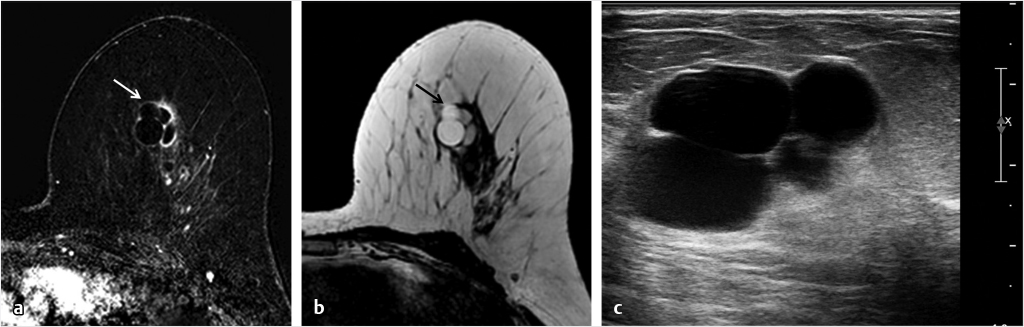
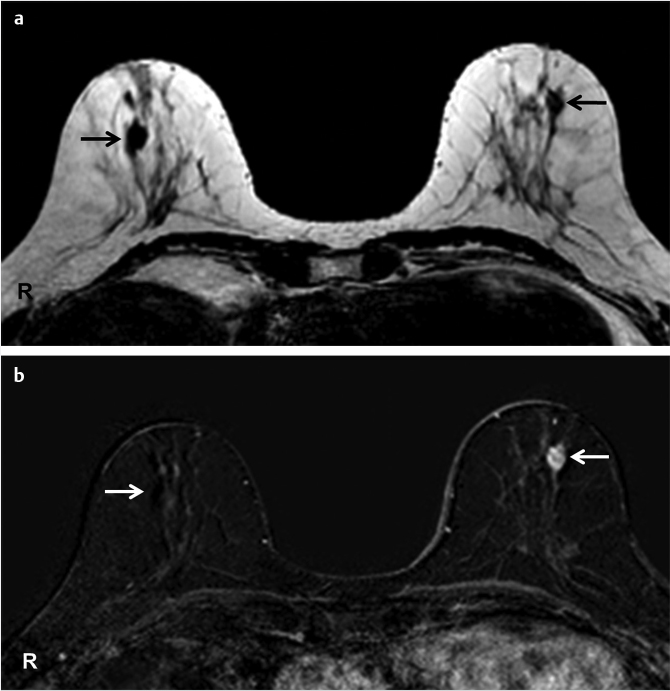
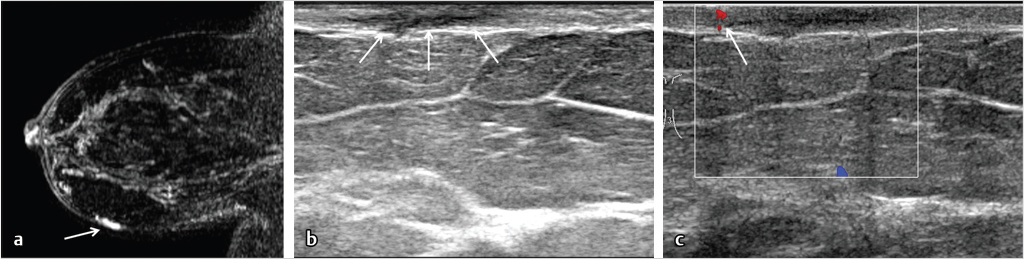
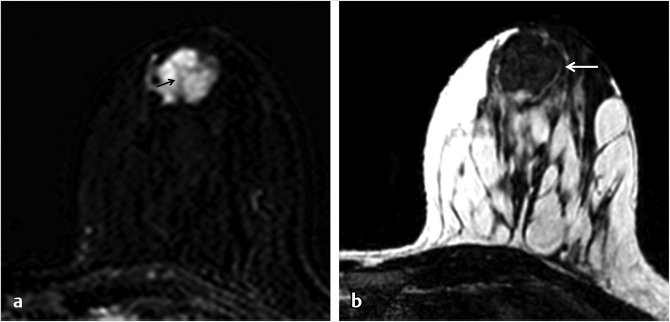
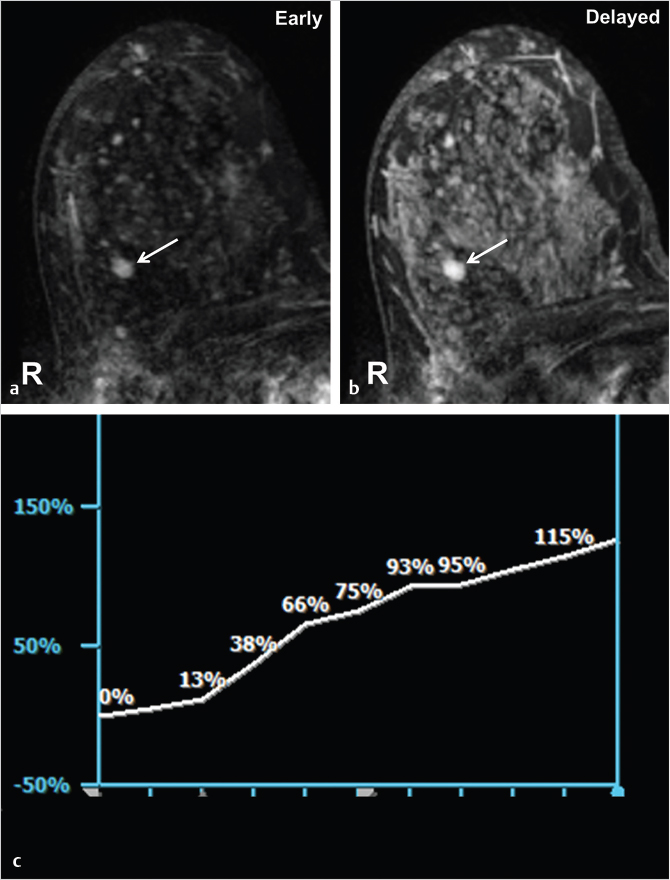
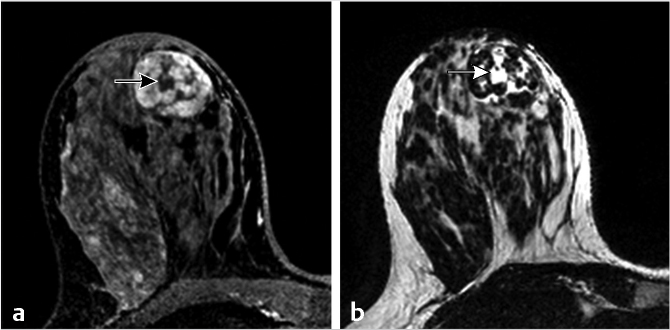
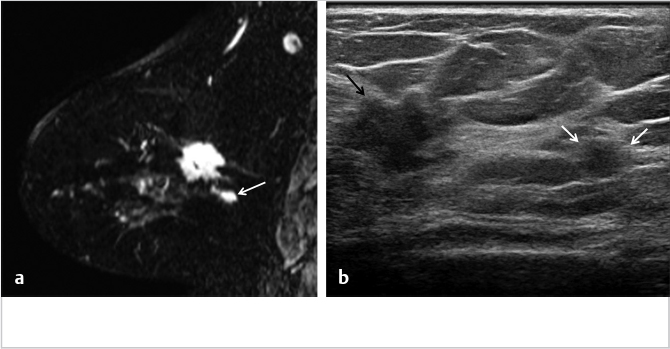
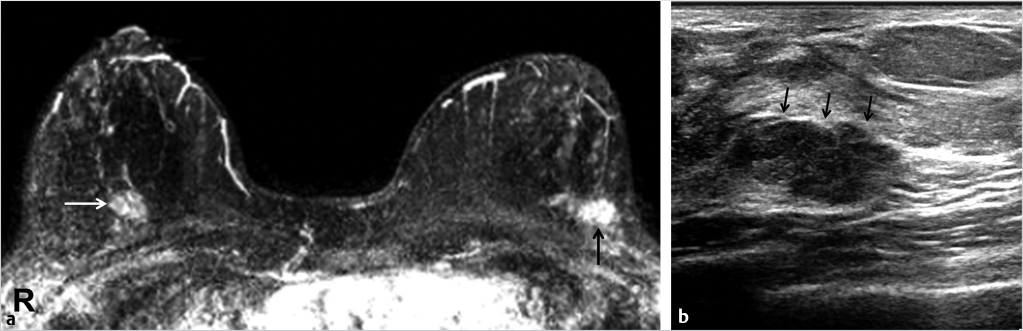
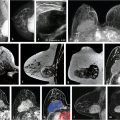
Fig. 9.1 Nodular parenchymal enhancement. Multiple enhancing foci are distributed in both breasts on MIP image (a) and on postcontrast axial T1-weighted subtraction image (b). The distribution appears asymmetric between the breasts, but the enhancing foci are distributed within the parenchyma, as is confirmed by comparison to axial T2-weighted image (c).Fig. 9.2 Intramammary lymph node. An enhancing focus associated with a suggestion of small area of nonenhancing area (arrow) is present in the left posterior inner breast on postcontrast axial T1-weighted subtraction image (a). On the same slice of axial T2-weighted image (b), the nonenhancing area (arrow) shows fat signal, consistent with fatty hilum of intramammary lymph node.Fig. 9.3 Multiple similar-shaped and similar-sized lesions. There are multiple similar-shaped and similar-sized masses (arrows) in the left breast in postcontrast axial T1-weighted subtraction image (partial MIP image). These masses were stable for 3 years.Fig. 9.4 Thin, regular rim enhancement. A rim enhancing lesion (white arrow) is present in the left breast on postcontrast axial T1-weighted subtraction image (a). The rim enhancement is smooth and thin. On the axial T2-weighted image (b), the lesion (arrow) shows homogenous water signal. Focused ultrasound (c) confirms it to be a simple cyst.Fig. 9.5 Nonenhancing lesion (with an enhancing lesion for comparison). Axial T2-weighted image (a) demonstrates a low signal mass in each breast (black arrows). On postcontrast axial T1-weighted subtraction image (b), the mass on the right breast does not enhance at all (white arrow), consistent with benign pathology (fibroadenoma). The mass in the left breast shows a thick, rim enhancement, suggesting malignant lesion (white arrow). This left breast mass was later proven to be malignant (invasive ductal carcinoma) by percutaneous biopsy.Fig. 9.6 Skin lesion; an enhancing lesion is usually benign. There is an enhancing lesion (arrow) in the lower portion of the breast on postcontrast sagittal T1-weighted subtraction image (a). Ultrasound (b) confirms that the lesion has the typical appearance of sebaceous cyst, located within the skin layer (white arrows). Mild blood flow (white arrow) on color Doppler image (c) suggests that there is mild inflammation.Fig. 9.7 Enhancing mass with dark internal septations. An oval enhancing mass with dark internal septations (small black arrow) is present in the left anterior breast on postcontrast axial T1-weighted subtraction image (a). Axial T2-weighted image shows a circumscribed low signal mass (b, white arrow). Ultrasound of this lesions shows a circumscribed homogeneously hypoechoic mass, suggesting fibroadenoma, which was confirmed by ultrasound-guided biopsy.Fig. 9.8 Slowly enhancing, circumscribed mass. A circumscribed, oval mass (white arrow) is enhancing slowly in the right breast on postcontrast axial T1-weighted subtraction image (a, b). Magnitude of enhancement is obviously higher on the delayed phase (b) than on the early phase (a). Kinetic curve (c) shows slow initial uptake and persistent pattern. The mass was stable for 2 years with ultrasound follow-up.Fig. 9.9 Fat-containing lesion. A circumscribed, round mass showing heterogeneous internal enhancement is present in the right breast on postcontrast axial T1-weighted fat-suppression image (a). Nonenhancing components on T1-weighted image (a, black arrow) correspond to areas of fat signal (white arrow) on axial T2-weighted image (b). This lesion is consistent with a benign fibroadenolipoma.Fig. 9.10 Small linear NME (nonbranching). A linear nonmass enhancement (9 mm) was newly detected in a high-risk woman (strong family history of breast cancer) on postcontrast axial and sagittal T1-weighted subtraction image (a, b, white arrow). This nonmass enhancement is less than 1 cm and nonbranching type. The lesion was proven to be benign with subsequent MRI-guided biopsy.Fig. 9.11 Staging MRI for known cancer, with unexpected satellite lesion. A 47-year-old woman with biopsy-proven cancer (invasive lobular carcinoma) in the right breast. Staging MRI shows a satellite lesion (white arrow) posterior and inferior to the known cancer on postcontrast axial T1-weighted subtraction image (a). MR-directed ultrasound shows a correlating mass (b, white arrows) posterior to the index malignancy (black arrow). This satellite lesion was proven to be malignant (invasive lobular carcinoma) upon a surgical excision. Being a lesion in the same quadrant as that of a known cancer, the lesion should be treated as malignant until proven otherwise, unless there are definite signs of benignity.Fig. 9.12 Staging MRI for known cancer, with unexpected contralateral lesion. A 47-year-old woman with biopsy-proven cancer (invasive ductal carcinoma, grade 1) in the left breast (black arrow). An unexpected enhancing mass (white arrow) is present on postcontrast axial T1-weighted subtraction MIP image (a). MR-directed ultrasound shows a correlated mass (black arrows) in the right breast (b). Ultrasound-guided biopsy of this right breast mass revealed DCIS, grade 1.Fig. 9.13 Typical malignant lesion detected on high-risk screening. The patient was a 61-year-old BRCA 1 mutation carrier. A new, irregular-shaped, speculated enhancing mass (white arrow) is present on postcontrast axial T1-weighted subtraction image (a). MR-directed ultrasound shows a correlated irregular hypoechoic mass with thick echogenic rim (b, black arrows).
9.2 Follow-up for Probably Benign Lesions
There are no systematic methods for differentiating probably benign lesions from suspicious lesions. Published articles generally report that a BI-RADS 3 assessment made by experienced radiologists may result in a malignancy rate of 2 to 3%. Follow-up MRI is usually performed after 6 months when a BI-RADS 3 assessment is made, with short-term follow-up usually continuing at 6, 12, and 24 months, as long as the lesion does not change in appearance. Two-year stability of the lesion is usually considered to be sufficient for a benign diagnosis. If the lesion appears smaller or less enhancing, or if it disappears during the follow-up period, it can be downgraded as benign. A decision to downgrade a lesion must be made prudently, as the change in appearance of a lesion can be easily influenced by various factors: the injection rate/volume of contrast, differences in magnetic field strength, or even the patient’s positioning. On the other hand, if a lesion shows an increase in size or a change in its kinetic pattern from a benign to a suspicious pattern, a biopsy should be performed.
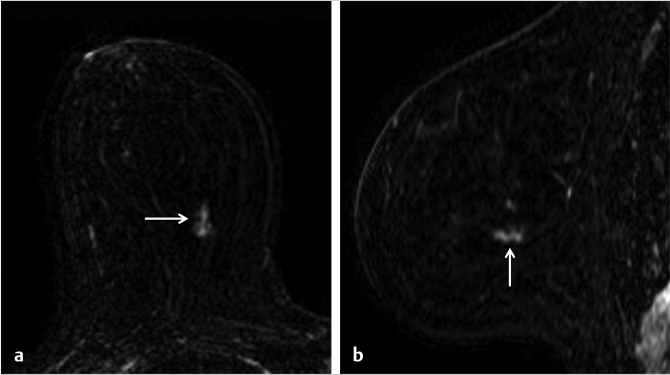
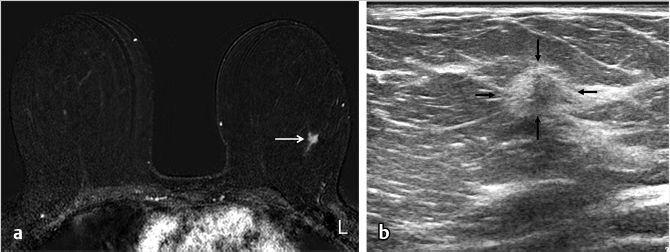
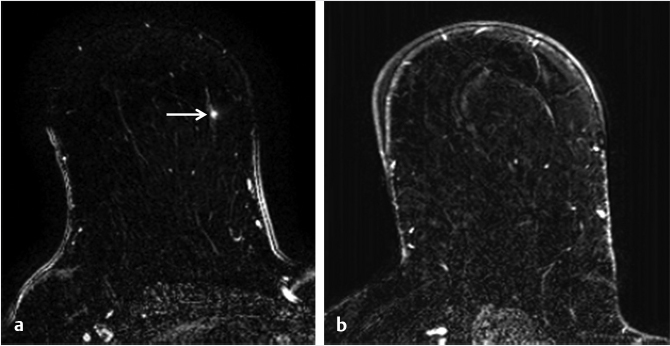
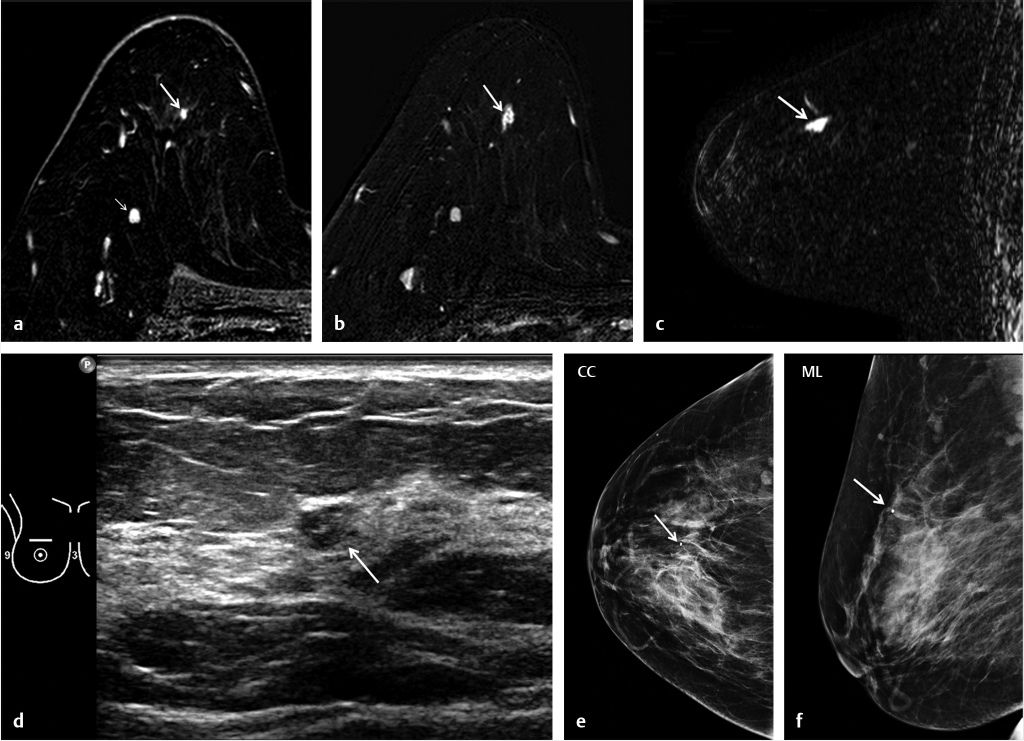
Fig. 9.14 Short-term follow-up, benign lesion. A new enhancing focus (arrow) was demonstrated on postcontrast axial T1-weighted subtraction image (a) in a screening MRI of 47-year-old BRCA 1-positive woman with strong family history of breast cancer. Short-term follow-up MRI was performed 6 months later (b). The enhancing lesion was no longer present in the follow-up MRI, and the lesion was diagnosed to be benign.Fig. 9.15 Short-term follow-up, malignant lesion. A new enhancing focus (white arrow) was demonstrated on postcontrast axial T1-weighted subtraction image (a) in a screening MRI of 49-year-old woman with personal history of left breast cancer. There was a stable intramammary lymph node in the same breast (small white arrow). Short-term follow-up MRI was performed 6 months later. The lesion shows interval enlargement, associated with rim enhancement (white arrow), on follow-up postcontrast axial and sagittal T1-weighted subtraction images (b, c). MR-directed ultrasound found a correlating 5-mm mass (d, white arrow). Two views of postbiopsy mammogram (e, f) demonstrate a marker clip (arrow) to be placed in approximately the same location as the target tumor on MRI (b, c). Ultrasound-guided biopsy revealed invasive ductal carcinoma grade 3 with high-grade DCIS. The final pathology of the surgical specimen revealed the lesion had 3-mm invasive component, and there was no lymph node metastasis.
9.3 How to Work Up Suspicious Lesions Initially Detected on MRI
A percutaneous biopsy should be performed for any suspicious lesion. The work-up process and the biopsy method may vary, according to the lesion type (focus, mass or nonmass enhancement [NME]). The mainstay biopsy method for such lesions is MRI-guided biopsy. Conventional imaging can be used in some cases in order to avoid an MRI-guided biopsy, which is expensive, time-consuming, and uncomfortable for some patients.
First of all, one should review the most recent mammogram to search for any lesion that might correlate with the MR findings (subtle calcification or asymmetry or lymph nodes). If there is a finding seen that is amenable for biopsy, then a stereotactic biopsy should be considered. If the mammogram does not reveal a possible correlate, then MR-directed (second-look) ultrasound is the next option. There is variability in the rate of detection of MR-detected findings on ultrasound, depending on the MR lesion type (focus, mass, NME). In general, masses are most likely to be correlated with MRI, but a focus and NME are not. One study reports that the correlation rates of mass, focus, and NME are 67, 46, and 12%, respectively. The overall correlation rate was 57.5% (1,266/2,201) in one review series.
9.3.1 Focus
MRI-guided biopsy is the first choice for work-up, because it is not easy to correlate a focus with MR-directed ultrasound. There are, however, some exceptions. It is worth attempting an MR-directed ultrasound if a focus is in close proximity to a visible anatomic landmark lesion or structure. A landmark, for example, could be a known mass, a cyst, a surgical seroma, the nipple, etc. If there are such landmarks near the target, an ultrasound study could be performed, focused on a specific region for detection and biopsy.
9.3.2 Mass
It is worth trying to perform an MR-directed ultrasound for any kind of mass.
Only gold members can continue reading. Log In or Register to continue