Chapter 110 Trauma in children accounts for more than 500,000 hospital admissions and 20,000 deaths per year. After cranial trauma, the abdomen is the second most common site of injury, and approximately 80% of abdominal injuries are due to blunt force trauma. The most common reported mechanism is motor vehicle crashes, followed by automobile–pedestrian injuries. Other common causes of injury include bicycle trauma and falls from a height. In young children, injuries also may result from intentional or nonaccidental trauma.1 Clinical variables that have been associated with a high risk of injury include gross hematuria, abdominal tenderness, seat belt ecchymoses, and a low trauma score. Seat belt ecchymoses across the lower abdomen or flank represent an important high-risk marker for injury.2,3 Such ecchymoses are associated with a complex of injury to the lumbar spine, bowel, and bladder that accounts for most injuries to belted motor vehicle passengers. The rapid and accurate evaluation of injured children with CT has resulted in improved triage, has contributed to reduced morbidity and mortality, and along with improvements in supportive care, has played a critical role in the success of nonoperative management of solid organ injuries. CT findings have been shown to change the initial management plan in nearly half of children assessed after blunt abdominal trauma.4–6 Sonography remains widely used in the screening of injured children and adults and has been shown to have high sensitivity and specificity in the detection of hemoperitoneum; however, its utility is limited in comparison with CT. Solely identifying fluid does not necessarily reveal the cause or the site of injury, and the presence of hemoperitoneum in a hemodynamically stable child typically does not affect clinical management decisions. Furthermore, sonography provides no diagnostic information regarding injury to the bony pelvis or lumbar spine, it cannot be used in the diagnosis of hollow viscus injury, and it has been shown to miss approximately one fourth to one third of solid organ injuries.7 Thus if one relies on identification of peritoneal fluid as a marker for hepatic and splenic injury, one will miss a significant number of injuries. Nevertheless, sonography has a potential role in diagnosing hemodynamically unstable patients because it can be performed rapidly at the bedside before the patient is taken to the operating room. In this role, it serves as a fast, noninvasive replacement for diagnostic peritoneal lavage. Recent studies suggest that contrast-enhanced sonography may have improved accuracy in delineating solid organ injuries.8 The liver is the most frequently injured viscus after blunt trauma in children, in whom this organ is poorly protected from injury by overlying ribs because the immature chest wall is easily deformed by external forces. A hepatic laceration appears as a nonenhancing region of varying configuration (Fig. 110-1) that may be linear or branching. Lacerations may be associated with a parenchymal or a subcapsular hematoma. Figure 110-1 Hepatic laceration and hemoperitoneum. The liver is surrounded by a thin capsule that in turn is covered by a peritoneal reflection of thin connective tissue. The presence of hemoperitoneum associated with hepatic injury principally relates to violation of the liver capsule at the site of injury. In several large series, hepatic injury was associated with hemoperitoneum in approximately two thirds of cases. Associated hemoperitoneum may be seen throughout the greater peritoneal cavity. Often the largest fluid pockets are located in the pelvis. Hepatic injury may not be associated with intraperitoneal hemorrhage if the injury does not extend to the surface of the liver, if the hepatic capsule is not disrupted, or if the injury extends to the liver surface in the bare area of the liver, which is devoid of peritoneal reflection (Fig. 110-2). Injury that extends to the bare area may lead to associated retroperitoneal hemorrhage, with blood often surrounding the right adrenal gland or extending into the anterior pararenal space. Figure 110-2 Hepatic laceration without hemoperitoneum. Circumferential zones of periportal low attenuation may be seen in the liver after trauma. The presence of these low attenuation zones does not indicate hepatic injury. They most likely represent distended periportal lymphatics as a result of intravascular third-space fluid losses that occur after fluid resuscitation.9,10 Treatment: A number of grading scales have been proposed to quantify the severity of hepatic injury. These scales emphasize the anatomic extent of the injury, including capsular integrity, extent of subcapsular collection, extent of parenchymal disruption, and involvement of the vascular pedicle. The most widely used grading scale was developed by the American Association for the Surgery of Trauma. It was devised initially to reflect surgical findings but often is used to report severity of organ injury upon CT scanning. In children, these scales are not predictive of the need for operative management because in the vast majority of hepatic injuries, bleeding typically stops spontaneously and the injuries can be managed successfully without surgery regardless of the severity.11 This response likely is a result of the relatively smaller size of blood vessels and the enhanced vasoconstrictive response in children relative to adults. Between 1% and 3% of children with hepatic injury require surgical or endovascular hemostasis. However, injury grading scales often are used in the decision algorithm of patient management regarding intensity and length of hospitalization and activity restriction. Splenic injury also is common after blunt trauma and frequently is associated with other organ injuries (Fig. 110-3). Because the spleen is much smaller than the liver, complex injury results in shattering or fragmentation of the organ (Fig 110-4). Associated intraparenchymal or subcapsular hematoma may be present. As with hepatic injury, associated intraperitoneal hemorrhage is not always present, especially when the splenic capsule remains intact. Absence of hemoperitoneum is observed in approximately 25% of splenic injuries. After injury involving the splenic hilum, blood also can track along the splenorenal ligament into the anterior pararenal space surrounding the pancreas. Figure 110-3 Hepatic, splenic, and renal injury. Figure 110-4 A shattered spleen. Treatment: Various injury grading scales have been described to objectively quantify injury to the spleen. As is true for hepatic injury, these scales are not predictive of surgical treatment in children because bleeding typically stops spontaneously and nonoperative management is successful in most splenic injuries.11,12 Grade of injury often is used for nonoperative clinical decision making, similar to the use of grading in hepatic injury.12–14
Abdominal Trauma
Overview
Clinical Presentation
Imaging
Sonography in the Assessment of Abdominal Trauma
Computed Tomography Findings
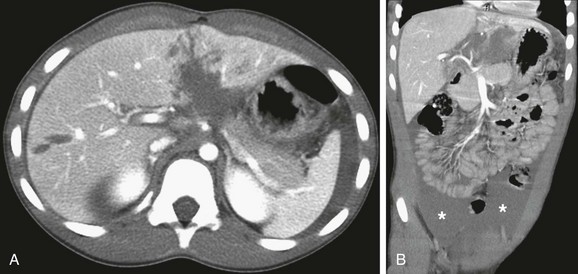
Contrast-enhanced axial computed tomography scan through the upper abdomen (A) reveals a complex hepatic laceration involving segment four and a simple laceration of segment 5. A coronal reformat image (B) shows a large associated hemoperitoneum in the pelvis (asterisk).

Coronal reformat of a contrast-enhanced computed tomography scan reveals a laceration of segment 8. No associated hemoperitoneum is present.
Splenic Injury

A contrast-enhanced axial computed tomography scan through the upper abdomen reveals a laceration to segment 3 of the left hepatic lobe (white arrow), a splenic hematoma (arrowhead), and a small laceration to the left kidney (black arrow).

A contrast-enhanced axial computed tomography scan through the upper abdomen shows a shattered spleen with only a small amount of central contrast enhancement. Note right perihepatic hemoperitoneum (arrowheads).
Abdominal Trauma








