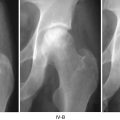
Fig. 36.1
Comparison of alendronate and placebo
Table 36.1
Radiographic evaluation (University of Pennsylvania System)
Fosamax | |||||||
Stage | 0 | I | IIC | IIIC | IV | V and VI | THA |
Baseline | – | – | 20 | 12 | – | – | – |
Follow-up | 0 | 0 | 11 | 11 | 9 | 1 | 4 |
Placebo | |||||||
Stage | 0 | I | IIC | IIIC | IV | V and VI | THA |
Baseline | – | – | 25 | 8 | – | – | – |
Follow-up | 1 | 0 | 14 | 9 | 9 | 0 | 5 |
Table 36.2
MRI evaluation and Harris Hip Score
% of the area of osteonecrosis in femoral head | Alendronate (N) | Placebo (N) | p-valuea |
|---|---|---|---|
Baseline | 47.0 ± 19.4 (32) | 45.8 ± 19.4 (30) | 0.6262 |
End of study/THA/withdrew | 37.9 ± 19.9 (26) | 38.8 ± 16.6 (22) | 0.8920 |
Difference | −6.6 ± 11.9 (26) | −6.6 ± 13.9 (19) | 0.5170 |
95 % C.I. | −11.4 to −1.8 | −13.3–0.1 | |
Harris Hip Score (subject no.) | 26 | 26 | |
Baseline | 78.1 ± 12.5 | 76.6 ± 15.2 | 0.6804 |
Follow-up | 79.3 ± 14.2 | 83.8 ± 12.8 | 0.2435 |
Table 36.3
Short Form-36
Dimension | Alendronate | Placebo | p-valuea | ||
|---|---|---|---|---|---|
N | 31 | 28 | |||
Baseline | Mean ± SD | Medium | Mean ± SD | Medium | |
Physical functioning | 60.3 ± 24.8 | 60.0 | 58.0 ± 28.1 | 55.0 | 0.7388 |
Role limitation due to physical problem | 46.0 ± 40.4 | 50.0 | 50.9 ± 44.9 | 62.5 | 0.6588 |
Bodily pain | 58.5 ± 20.5 | 57.5 | 56.6 ± 24.2 | 62.5 | 0.7401 |
General health | 56.0 ± 17.8 | 55.0 | 53.4 ± 20.5 | 55.0 | 0.6074 |
Vitality | 60.5 ± 20.3 | 55.0 | 52.3 ± 23.7 | 52.5 | 0.1598 |
Social functioning | 70.2 ± 24.7 | 75.0 | 65.6 ± 26.3 | 68.8 | 0.4972 |
Role limitation due to emotional problem | 58.1 ± 44.7 | 66.7 | 60.7 ± 43.6 | 83.3 | 0.8188 |
Mental health | 65.5 ± 17.0 | 68.0 | 61.6 ± 21.5 | 64.0 | 0.4310 |
Total score | 59.2 ± 18.6 | 55.9 | 57.0 ± 21.9 | 60.1 | 0.6788 |
N | 30 | 28 | |||
The end of study/THA/withdrew | Mean ± SD | Medium | Mean ± SD | Medium | |
Physical functioning | 55.0 ± 26.2 | 52.0 | 56.1 ± 27.2 | 55.0 | 0.8742 |
Role limitation due to physical problem | 37.5 ± 43.4 | 0.0 | 38.4 ± 42.7 | 12.5 | 0.9374 |
Bodily pain | 58.1 ± 20.4 | 57.5 | 63.3 ± 18.6 | 67.5 | 0.3140 |
General health | 51.0 ± 20.4 | 45.0 | 50.8 ± 23.8 | 50.0 | 0.9731 |
Vitality | 53.5 ± 18.1 | 50.0 | 54.8 ± 20.1 | 52.5 | 0.7931 |
Social functioning | 64.2 ± 20.2 | 68.8 | 63.8 ± 24.4 | 50.0 | 0.9556 |
Role limitation due to emotional problem | 50.0 ± 47.7 | 50.0 | 53.6 ± 46.6 | 62.5 | 0.7743 |
Mental health | 60.7 ± 15.9 | 60.0 | 61.1 ± 19.5 | 60.0 | 0.9189 |
Total score | 53.3 ± 20.2 | 53.7 | 54.7 ± 21.9 | 61.3 | 0.8011 |
Difference of dimension | Alendronate | Placebo | p-valuea |
|---|---|---|---|
N | 30 | 28 | |
Mean ± SD | Mean ± SD | ||
Physical functioning | −5.8 ± 26.3 | −1.9 ± 30.8 | 0.6024 |
Role limitation due to physical problem | −10.0 ± 43.8 | −12.5 ± 45.4 | 0.8318 |
Bodily pain | −1.3 ± 21.2 | 6.7 ± 22.4 | 0.1656 |
General health | −5.8 ± 19.8 | −2.6 ± 22.6 | 0.5621 |
Vitality | −8.5 ± 18.9* | 2.5 ± 18.2 | 0.0288 |
Social functioning | −7.9 ± 21.4 | −1.7 ± 20.6 | 0.2718 |
Role limitation due to emotional problem | −10.0 ± 51.9 | −7.1 ± 39.9 | 0.8160 |
Mental health | −5.8 ± 17.4 | −0.42 ± 14.4 | 0.2027 |
Total score | −6.9 ± 19.3* | −2.2 ± 15.4 | 0.3137 |
Our primary goal was to evaluate whether Aln can decrease the need for THA. Both surgical and nonsurgical approaches have been developed to preserve the joint and are used in an attempt to arrest the progression of disease, as well as to offer pain relief [39, 40]. Maintenance of the femoral head shape and articular surface, and halting the progression of the disease, appears to be one of the preferred methods of avoiding arthrosis of the hip joint. Surgical treatments with osteotomies and/or bone grafts that restore and revive the femoral head provide excellent long-term results [1, 39, 41–43]. Medication that prevents the early collapse of the osteonecrotic femoral head is an attractive treatment. Using Aln in an attempt to slow down the bone remodeling process had been reported by Lai et al. [11]. In a randomized, control, prospective study, they showed the effectiveness of Aln in delaying or even avoiding THA in pre-collapse femoral heads. In the study by Agarwala et al., THA was circumvented with early use of Aln in pre-collapse femoral heads [10, 13]. In terms of our primary goal, the result was different from the above studies [11, 13]. We did not find any obvious effect of Aln in decreasing the possibility of receiving THA. Hip arthroplasty for ON is dependent on the patient’s pain severity and functional needs; therefore, the disease status and the functional demand of the patient are very important factors in terms of treatment options. It is important that any decision to perform arthroplasty should be supported by robust clinical information. A double-blind design is very important because the disease course sometimes involves subjective judgment by the investigator and the expectations of individual patients when making decisions concerning undergoing surgical treatment. No standard criteria for the timing of surgical treatment have been defined. A meta-analysis of the outcomes of protected weight bearing in 819 patients demonstrated a failure rate of >80 % at a mean of 34 months [44]. Even though all patients had a large lesion (>30 %) in our study, we found a very low incidence of THA (13.06 % in the Aln group and 15.60 % in the placebo group) due to the collapse of the femoral head, as compared with the previous literature [1, 40, 44–48]. In our study, all patients received daily oral calcium (500 mg) and vitamin D (400 IU). There is no report about the therapeutic effects of calcium and vitamin D. We are not certain of the reasons for the low incidence of THA and progression of disease in the placebo group. Because there is no data about the natural course of ON in the Taiwanese population, we are not certain as to whether there might be a racial difference in the natural course of ON. As such, there was a numerical reduction in the rate of THA in the Aln group compared with placebo that did not achieve statistical significance; this was likely because the study was originally designed to detect a between-group difference based on event rates of 35.7 % (10/28) and 3.4 % (1/29) in the placebo and Aln groups, respectively.
Related posts:
 Ischemia and Reperfusion Injury in Bone
Ischemia and Reperfusion Injury in Bone
 The University of Pennsylvania Classification of Osteonecrosis
The University of Pennsylvania Classification of Osteonecrosis
 Alumina Ceramic-on-Highly Cross-Linked Polyethylene Bearing in Cementless Total Hip Arthroplasty in Young Patients with Osteonecrosis of Femoral Head
Alumina Ceramic-on-Highly Cross-Linked Polyethylene Bearing in Cementless Total Hip Arthroplasty in Young Patients with Osteonecrosis of Femoral Head
 Impaction Bone Grafting
Impaction Bone Grafting
 Causes of Pain in Early and Advanced Stage Osteonecrosis
Causes of Pain in Early and Advanced Stage Osteonecrosis
 Kienböck’s Disease of the Lunate
Kienböck’s Disease of the Lunate
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


