Fig. 1
A patient with standard-risk medulloblastoma. This patient was simulated using a 1.5 mm CT slice thickness. Note the coverage of the cribriform plate as part of the target volume (the dark blue line is the PTVCSI, while the inner red line is the CTVCSI). Also note the PTVtbboost (purple line), CTVtbboost (orange line), and GTV (shaded purple) contours. Note that the CTV margin anteriorly in the brainstem is less compared to the posterior and lateral margins
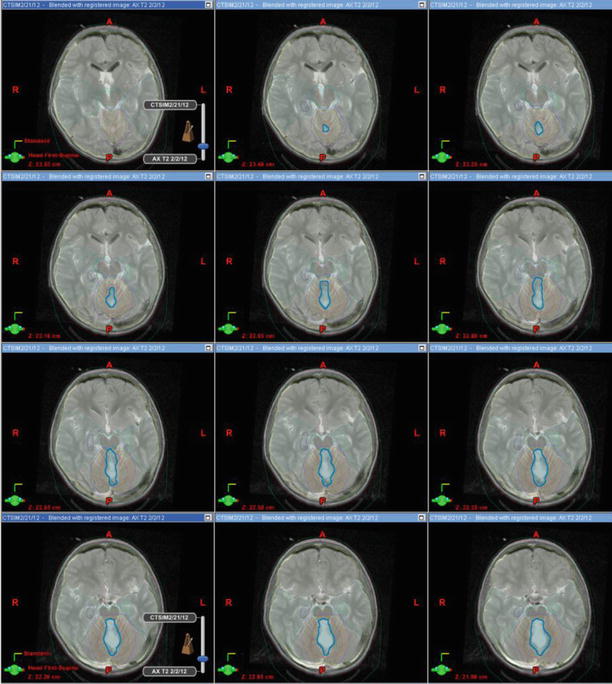
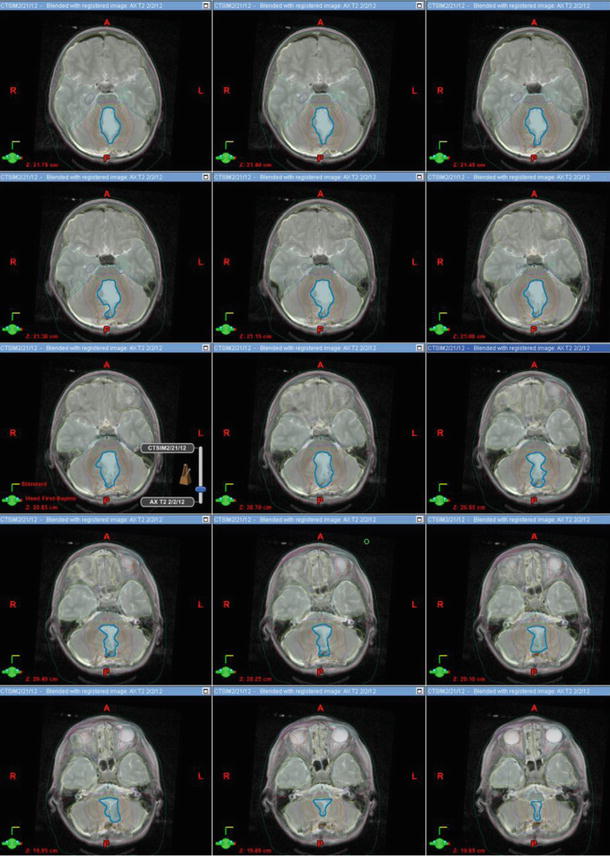
Fig. 2
MRI slices fused to CT simulation images from a similar patient who had a gross total resection of a medulloblastoma. This is an example of a tumor bed boost. The GTV (resection cavity) is shown in blue, CTVtbboost in light orange, and PTVtbboost in purple
Table 1
Recommended target volumes for the craniospinal (CSI) portion of the treatment
Target volumes | Definition and description |
|---|---|
GTV | Tumor bed includes all gross disease and the walls of the resection cavity as noted on the MRI. Surgical defects caused by the procedure (the route to and from the tumor bed) are not considered part of the cavity |
CTVCSI | The entire volume contained by the dura matter and in contact with the cerebrospinal fluid is the CTV. The cribriform plate should be included in the CTV. Because the spinal cord can in theory move in the canal, the CTV is defined as limits of the spinal canal down to the thecal sac termination as defined by the spinal MRI |
PTVCSI | CTV + 3–10 mm, depending on comfort level of daily patient positioning and institutional experience |
Table 2
Recommended target volumes of the tumor bed boost within the posterior fossa
Target volumes | Definition and description |
|---|---|
GTV | Tumor bed includes all gross disease and the walls of the resection cavity as noted on the MRI. Surgical defects caused by the procedure (the route to and from the tumor bed) are not considered part of the cavity |
CTVtbboost | CTVtbboost should include the entire GTV with a 1–1.5 cm margin |
Clinical limits to CTV expansion include the normal anatomic barriers to tumor spread such as the brainstem, the bone, and the tentorium. If there is brainstem invasion, then a portion of the brainstem in included in the CTV | |
PTVtbboost | CTVtbboost + 3–5 mm, depending on institutional experience |
Table 3
Recommended target volumes for the entire posterior fossa boost
Target volumes | Definition and description |
|---|---|
GTV | Tumor bed includes all gross disease and the walls of the resection cavity as noted on the MRI. Surgical defects caused by the procedure (the route to and from the tumor bed) are not considered part of the cavity |
CTVpf | CTVpf should include the posterior fossa. The brainstem is included in the posterior fossa compartment |
Clinical limits to CTV expansion include the normal anatomic barriers to tumor spread such as the bone and the tentorium | |
PTVpf | CTVpf + 3–5 mm, depending on institutional experience |
In the case of a growing child, the entire vertebral body must be contoured and included in the CTV when treating the craniospinal axis. An example is shown in Fig. 3. In a full-grown child or adult, the entire vertebral does not need to be included in the CTV. An example is shown in Fig. 4.
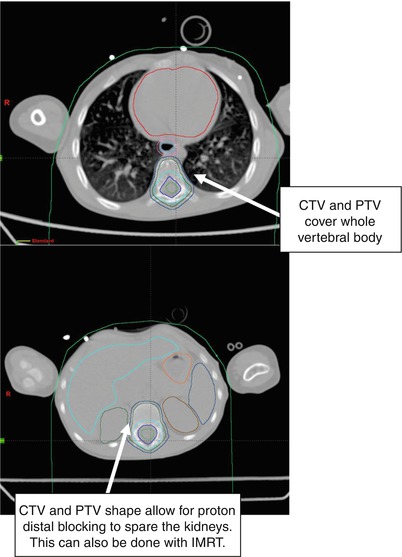
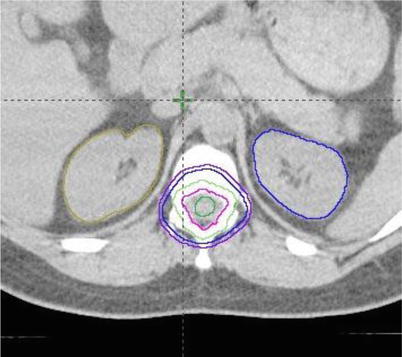
Fig. 3
Example of CTVs displayed on bone windows of the spine in a growing child. The CTV could cut across the vertebral body in a fully grown child or an adult
Fig. 4
This shows how the spine field changes for a fully grown patient. Note how the CTV (blue) and PTV (purple) lines are not outside of the bone anteriorly
Fusion of MR to CT is not perfect, so each slice of MR-based contours should ultimately be reviewed on the CT scan to make sure it is reasonable.
The standard recommendation for determining the caudal extent for the CTVCSI is to use the MRI scan to find the termination of the thecal sac. In the past the caudal margin has been set to the bottom of the S2 vertebral level; however, we now know that in one-third of cases, the termination will be higher or lower than S2. Going more inferiorly than necessary may deliver more exit dose into the gonads. When proton therapy is used for the craniospinal axis, the exit dose to the gonads is not of concern.
The current recommended dose to the craniospinal axis for standard-risk disease is 23.4 Gy in 13 fractions while for high-risk disease is 36 Gy in 20 fractions. In both cases, the recommended total dose to the CTV boost volume is 54 Gy. An ongoing Children’s Oncology Group study is looking at reducing the CSI dose from 23.4 to 18 Gy in children <7 years of age with standard-risk disease.
For the boost field, an ongoing COG study is examining the question of the appropriate boost volume for medulloblastoma. In this study, the two types of boost volumes include the entire posterior fossa (CTVpf) versus the tumor bed with a margin (CTVtbboost). Several single institutional studies have been published that support the safety and efficacy of the tumor bed boost. Normal anatomic constraints may limit the CTV boost volume in such a way that a uniform margin around the GTV is not necessary. The tentorium cerebelli (separates the posterior fossa and the supratentorial brain) and bony skull are considered as barriers of spread; therefore, the CTV should be limited not to extend beyond these barriers. Invasion into the brainstem is possible so expansion into the brainstem may be needed. In cases where the tumor is touching the brainstem, a limited margin of 2–3 mm has often been used for the anterior expansion of the CTV boost volume. In cases where tumor is not in contact with the brainstem such as in a case of a well-lateralized medulloblastoma, the brainstem is an anatomic barrier to spread and hence need not be included in the CTV boost volume (Figs. 5, 6, and 7).
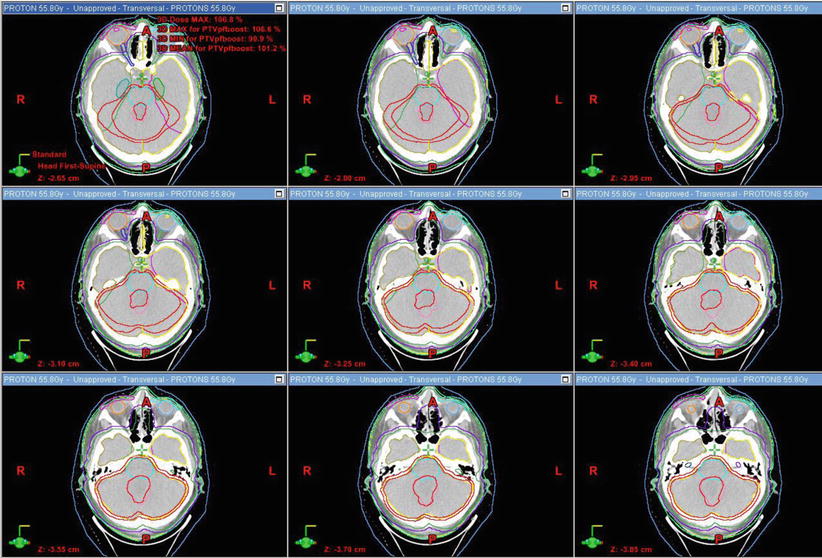
Fig. 5




The posterior fossa contours in a series of CT slices
Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
