Calcaneal Spurs
Anatomic Considerations
The calcaneus is the largest of the tarsal bones (Fig. 17.1). The main function of the calcaneus is to transfer the weight of the body to the ground, as well as to serve as a lever for the muscles of the calf. The plantar surface of the calcaneus is elevated posteriorly to form the calcaneal tuberosity. The calcaneal tuberosity is depressed centrally, with lateral and medial processes. It is at the medial process that symptomatic calcaneal spurs most commonly occur. The plantar fascia is made up of thick, longitudinally oriented connective tissue that is tightly attached to the plantar skin. It attaches to the medial calcaneal tuberosity and then runs forward, dividing into five bands, one going to each toe (Fig. 17.2). The plantar fascia provides dynamic support to the arch of the foot, tightening as the foot bears weight.
Clinical Correlates
Calcaneal spurs are a common cause of heel pain (Fig. 17.3). Calcaneal spurs may be asymptomatic or symptomatic. When symptomatic, calcaneal spurs are usually seen in conjunction with plantar fasciitis. The clinical syndrome associated with symptomatic calcaneal spurs is characterized by pain and tenderness over the plantar surface of the calcaneus made immediately worse by dorsiflexion of the toes. Calcaneal spurs are thought to be caused by an inflammation of the insertional fibers of plantar fascia onto the medial tuberosity of the calcaneus (Fig. 17.4). Inflammation of these insertional fibers of the plantar fascia can occur alone or can be part of a systemic inflammatory condition, such as rheumatoid arthritis, plantar fasciitis, Reiter syndrome, or gout (Figs. 17.5 and 17.6). In some patients, suffering from symptomatic heel spurs, there does not appear to be an inflammatory basis for the patient’s pain symptomatology and the etiology of the pain appears to be entirely mechanical as is seen with patients with gait abnormalities that include an excessive heel strike. High-impact aerobic exercise also has been implicated.
Pain on palpation of the insertion of the plantar fascia on the plantar medial calcaneal tuberosity is a consistent finding in patients with calcaneal spurs as is exacerbation of pain with active resisted dorsiflexion of the toes. Patients suffering from calcaneal spurs will also exhibit pain on deep palpation of the plantar fascia, especially when the toes are dorsiflexed pulling the plantar fascia taunt. The pain of calcaneal spurs is most severe on taking the first few steps after having not borne weight and is made worse by prolonged standing or walking. The pain of symptomatic heel spurs is made worse by standing for long periods or by weight bearing and is often relieved by padding of the affected heel.
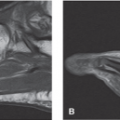
Compromise of the inferior calcaneal nerve, which is known as Baxter neuropathy produces medial heel pain similar to that of plantar fasciitis and calcaneal spurs. Causes of Baxter neuropathy, may occur because of plantar fasciitis, calcaneal spur, or secondary to internal foot derangement. Baxter neuropathy is diagnosed on MRI of the calcaneus which will demonstrate a distinctive sign of selective fatty atrophy of the abductor digiti minimi muscle (Fig. 17.7).
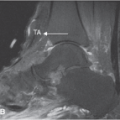
Plain radiographs are indicated in all patients who present with heel and foot pain (Figs. 17.8 and 17.9). Based on the patient’s clinical presentation, additional testing may be indicated, including complete blood cell count, sedimentation rate, and antinuclear antibody testing. MRI and/or ultrasound imaging of the ankle is indicated if calcaneal spurs, rupture of the plantar fascia, or joint instability is suggested (Figs. 17.10 to 17.13). Radionuclide bone scanning is useful to identify stress fractures of the calcaneus and foot, not seen on plain radiographs, and may aid in the diagnosis as there may be increased uptake of radionucleotide at the insertion of the plantar fascia at the calcaneus (Figs. 17.14 and 17.15).
Ultrasound Technique
To perform ultrasound evaluation of the calcaneus, the patient is placed in the prone position with the patient’s ankle hanging off the edge of the table. With the patient in the above position, a high-frequency linear ultrasound transducer is placed in a longitudinal plane with the inferior portion of the ultrasound transducer over plantar surface of the foot with the superior end of the transducer on the anterior portion of the calcaneus, and an ultrasound survey scan is taken (Fig. 17.16). The calcaneus, calcaneal spur, and linear plantar fascia are identified at its insertion on the calcaneus (Fig. 17.17). When the insertion of the plantar fascia is identified, it is evaluated for evidence of calcaneal spurs, insertional tendinopathy, and plantar fasciitis (Figs. 17.18 to 17.20).
 FIGURE 17.1 The calcaneus is the largest of the tarsal bones. The main function of the calcaneus is to transfer the weight of the body to the ground, as well as to serve as a lever for the muscles of the calf. (From Tank PW, Gest TR. The lower limb. In: Lippincott Williams & Wilkins Atlas of Anatomy. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:146.)
Related posts: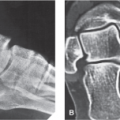 Arthritis and Other Abnormalities of the Subtalar Joint Arthritis and Other Abnormalities of the Subtalar Joint
 Arthritis and Other Abnormalities of the Ankle Joint Arthritis and Other Abnormalities of the Ankle Joint
 Anterior Tarsal Tunnel Syndrome and Other Abnormalities of the Deep Peroneal Nerve Anterior Tarsal Tunnel Syndrome and Other Abnormalities of the Deep Peroneal Nerve
 Retrocalcaneal and Achilles Bursitis Retrocalcaneal and Achilles Bursitis
 Hallux Valgus Deformity Hallux Valgus Deformity
 Plantar Fasciitis and Other Abnormalities of the Plantar Fascia Plantar Fasciitis and Other Abnormalities of the Plantar Fascia
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|