Anatomical location
Frequency (%)
Hip
200 (99)
Knee
179 (87)
Shoulder
146 (72)
Ankle
71 (35)
Elbow
17 (8)
Wrist
8 (4)
Calcaneus
6 (3)
Tarsal navicular
2 (1)
Cuneiform
1 (0.5)
Cuboid
1 (0.5)
Metacarpal head
1 (0.1)
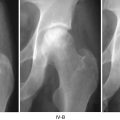
5.8 Stage Distribution at Time of Presentation
In a study on multifocal osteonecrosis [67], plain radiography or MRI revealed that most (69 %) joints presented in a precollapse stage. Eighty-five of 200 (43 %) hips had collapse (59 hips) or osteoarthritis (26 hips). Only 17 % of 179 knees, 38 % of 146 shoulders, and 24 % of 71 ankles had collapse or arthritis. Approximately 30 % of the lesions were diagnosed solely by MRI. There was a higher incidence of these asymptomatic lesions in the knee (38 %), shoulder (30 %), and ankle (44 %) than in the hip (18 %). The incidence of negative radiographic findings but positive MRI scans was highest in the ankle (44 %) and knee (38 %) and lower in the shoulder (30 %) and hip (18 %).
5.9 Summary
In summarizing the epidemiology of osteonecrosis in the USA, it is evident that the prevalence and incidence vary according to the risk factor of disease and the population being studied. Traumatic osteonecrosis is associated with specific fractures, and the incidence depends upon many factors such as age, displacement, type of fracture, and method of treatment. Nontraumatic ONFH can be idiopathic but is usually associated with corticosteroid usage, ethanol abuse, systemic lupus erythematosus, barotrauma, or marrow packing disorders such as sickle cell disease and Gaucher’s disease. The proportion of patients with steroid-related ONFH is increasing as solid organ and bone marrow transplantation are becoming more commonplace.
References
1.
Cleveland M, Fielding JW. A continuing end-result study of intracapsular fracture of the neck of the femur. J Bone Joint Surg Am. 1954;36-A:1020–30.PubMed
2.
3.
Haidukewych GJ, Rothwell WS, Jacofsky DJ, Torchia ME, Berry DJ. Operative treatment of femoral neck fractures in patients between the ages of fifteen and fifty years. J Bone Joint Surg Am. 2004;86-A:1711–6.PubMed
4.
5.
Swiontkowski MF, Winquist RA, Hansen Jr ST. Fractures of the femoral neck in patients between the ages of twelve and forty-nine years. J Bone Joint Surg Am. 1984;66:837–46.PubMed
6.
American Academy of Orthopaedic Surgeons. Orthopaedic Knowledge Update 7. Rosemont IL. AAOS 2002. p. 410–2.
7.
Crawford HB. Conservative treatment of impacted fractures of the femoral neck. A report of fifty cases. J Bone Joint Surg Am. 1960;42-A:471–9.PubMed
8.
Arnold WD, Lyden JP, Minkoff J. Treatment of intracapsular fractures of the femoral neck. With special reference to percutaneous Knowles pinning. J Bone Joint Surg Am. 1974;56:254–62.PubMed
9.
10.
Phemister DB. Treatment of the necrotic head of the femur in adults. J Bone Joint Surg Am. 1949;31A:55–66.PubMed
11.
Chapman MW, Stehr JH, Eberle CF, Bloom MH, Bovill Jr EG. Treatment of intracapsular hip fractures by the Deyerle method. A comparative review of one hundred and nineteen cases. J Bone Joint Surg Am. 1975;57:735–44.PubMed
12.
13.
14.
Stewart MJ, Milford LW. Fracture-dislocation of the hip; an end-result study. J Bone Joint Surg Am. 1954;36:315–42.PubMed
15.
Brav EA. Traumatic dislocation of the hip. J Bone Joint Surg. 1962;44A:1115.
16.
17.
18.
Mack GR, Bosse MJ, Gelberman RH, Yu E. The natural history of scaphoid non-union. J Bone Joint Surg Am. 1984;66:504–9.PubMed
19.
Haliburton RA, Sullivan CR, Kelly PJ, Peterson LF. The extra-osseous and intra-osseous blood supply of the talus. J Bone Joint Surg Am. 1958;40-A:1115–20.PubMed
21.
Canale ST, Kelly Jr FB. Fractures of the neck of the talus. Long-term evaluation of seventy-one cases. J Bone Joint Surg Am. 1978;60:143–56.PubMed
22.
Fukushima W, Fujioka M, Kubo T, Tamakoshi A, Nagai M, Hirota Y. Nationwide epidemiologic survey of idiopathic osteonecrosis of the femoral head. Clin Orthop Relat Res. 2010;468:2715–24.PubMedCentralPubMedCrossRef
23.
Kang JS, Moon KH, Kwon DG, Shin BK, Woo MS. The natural history of asymptomatic osteonecrosis of the femoral head. Int Orthop. 2013;37:379–84.PubMedCentralPubMedCrossRef
Related posts:
 Distinguishing Bone Marrow Edema Syndrome from Osteonecrosis
Distinguishing Bone Marrow Edema Syndrome from Osteonecrosis
 The University of Pennsylvania Classification of Osteonecrosis
The University of Pennsylvania Classification of Osteonecrosis
 Alumina Ceramic-on-Highly Cross-Linked Polyethylene Bearing in Cementless Total Hip Arthroplasty in Young Patients with Osteonecrosis of Femoral Head
Alumina Ceramic-on-Highly Cross-Linked Polyethylene Bearing in Cementless Total Hip Arthroplasty in Young Patients with Osteonecrosis of Femoral Head
 Impaction Bone Grafting
Impaction Bone Grafting
 Causes of Pain in Early and Advanced Stage Osteonecrosis
Causes of Pain in Early and Advanced Stage Osteonecrosis
 Kienböck’s Disease of the Lunate
Kienböck’s Disease of the Lunate
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


