Key Points
- •
The primary indication to perform a point-of-care ultrasound exam of the kidney is to evaluate for hydronephrosis.
- •
Any suspicious mass detected by point-of-care ultrasound warrants further investigation and expert consultation.
- •
A bladder ultrasound exam should accompany every renal ultrasound exam. A distended bladder due to bladder outlet obstruction is a common cause of hydronephrosis.
Background
Renal ultrasound provides a fast, radiation-free, and cost-effective alternative to computed tomography (CT) for the initial workup of low-risk patients who present with acute symptoms ranging from undifferentiated abdominal pain to painless hematuria. Ultrasound is the imaging modality of choice for investigating obstructive uropathy in pregnant and pediatric populations, given the adverse effects of ionizing radiation.
Focused renal ultrasound can accurately detect and grade hydronephrosis in the context of obstructive uropathy, directly visualize large obstructing calculi, and characterize renal cysts or solid masses. Renal ultrasound can be incorporated into the assessment of any patient with undifferentiated flank or abdominal pain. When clinical suspicion for renal calculus is high, the presence of hydronephrosis on the side of pain can be considered as de facto evidence of obstructive uropathy. Sensitivity of ultrasound for detecting a calcified stone can be improved with the addition of a single plain film of the abdomen (kidneys, ureter, and bladder, or KUB). Severity of hydronephrosis observed may correlate with the duration of obstruction and possibly with the size of the obstructing calculus. When stone disease is clinically less likely or an alternate pathology such as abdominal aortic aneurysm, gallbladder disease, ovarian torsion, or ectopic pregnancy is being considered, the absence of hydronephrosis effectively guides investigations elsewhere.
Normal Anatomy
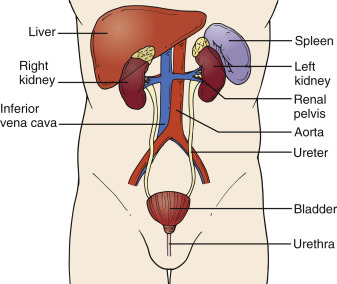
Kidneys are retroperitoneal organs that lie in an oblique longitudinal plane with the inferior pole of each kidney more anterior and lateral compared to its superior pole ( Figure 20.1 ). Therefore, the transducer must be positioned obliquely to image the kidney along its long axis. The left kidney is located more superiorly and posteriorly compared to the right kidney. The left kidney is usually visualized through the acoustic window provided by the spleen due to interference by bowel and stomach gas anteriorly, and the right kidney is often visualized through the acoustic window provided by the liver. The right kidney is slightly larger than the left kidney, but both kidneys are normally within 2 cm of each other in any dimension. Normal kidneys are 9–12 cm long, 4–6 cm wide, and 2.5–3.5 cm thick.
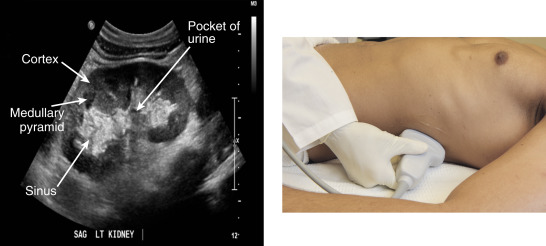
Kidneys are divided into two distinct anatomic parts: renal parenchyma and renal sinus ( Figure 20.2 ). Renal parenchyma is further subdivided into renal cortex and medulla. The medulla consists of cone-shaped medullary pyramids. Renal parenchyma surrounds the sinus on all sides except at the hilum. The hilum is where the renal artery, renal vein, and proximal ureter enter the renal sinus. Prominent fatty deposits within the renal sinus give it a hyperechoic appearance and distinguish it from the hypoechoic, grainy renal parenchyma. This difference in echogenicity is known as the sonographic double density of the kidney.
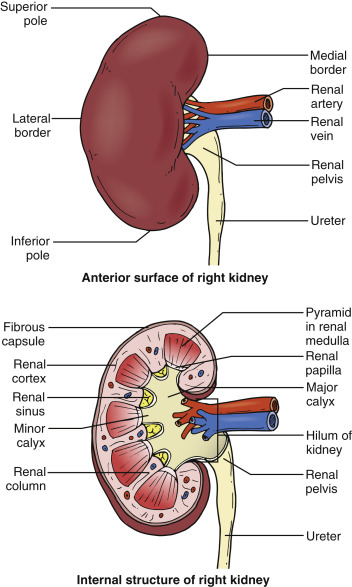
Image Acquisition
A low-frequency transducer with deep penetration, either phased-array or curvilinear type, is used to image the kidneys. The narrower beam width of a phased-array transducer is ideal for imaging between the ribs, but the wider beam width of a curvilinear transducer allows visualization of the entire kidney longitudinally in a single view.
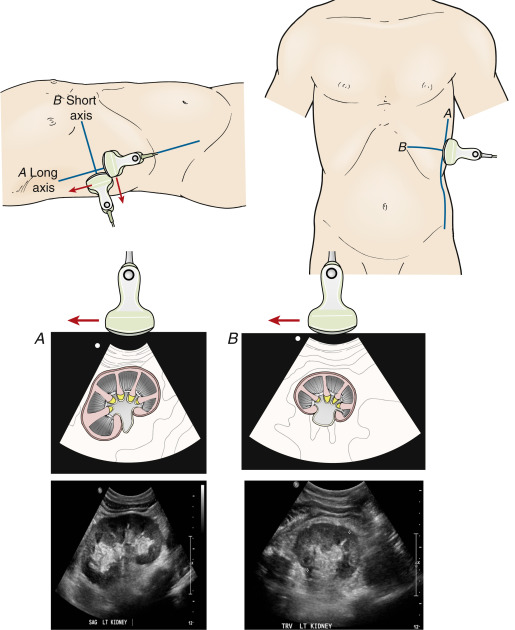
When scanning a patient with a suspected renal pathology, scan the unaffected side first to obtain a baseline image to compare with the affected side. To image the right kidney, place the patient in a supine position with the transducer in a coronal plane in the midaxillary to anterior axillary line at the level of the xiphoid process. Center the kidney on the screen and rotate the transducer 15-30 degrees counterclockwise to aim the transducer marker slightly posteriorly to capture a true long-axis view of the right the kidney. While holding the transducer in the same location on the skin surface, tilt or fan the transducer anteriorly and posteriorly to assess the entire kidney from its most anterior to posterior surface. Rotate the transducer 90 degrees counterclockwise from the long-axis view to obtain a transverse cross section of the kidney. Tilt or fan the transducer superiorly and inferiorly to assess the superior and inferior poles of the kidney. Figure 20.3 illustrates transducer positions to obtain long- and short-axis views of the kidney.
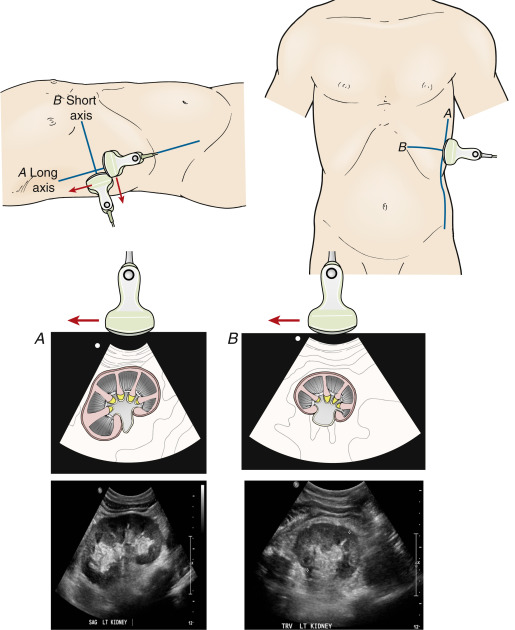
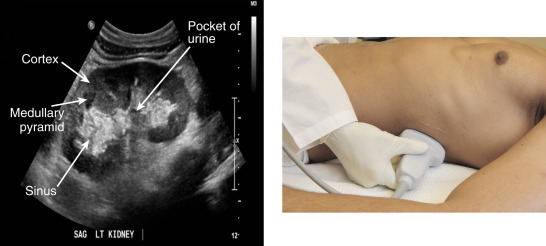
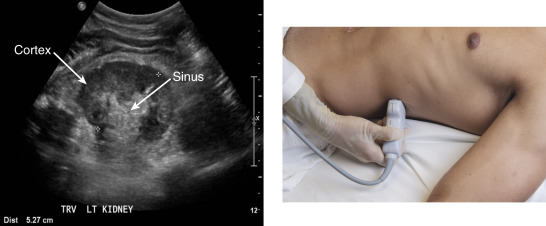
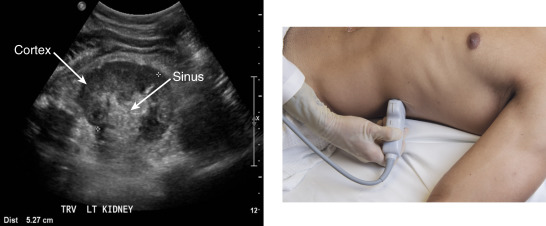
The left kidney is more posterior and superior than the right kidney. Placing the patient in a right lateral decubitus position facilitates visualization of the left kidney and reduces interference from the ribs and bowel gas. Requesting the patient to hold his breath in maximal inspiration will shift the kidney caudally to further reduce interference from rib shadows. Identify the left kidney with the transducer in a coronal plane on the posterior axillary line and then rotate the transducer 15-30 degrees clockwise aiming the transducer marker posteriorly to acquire a true long-axis view ( Figure 20.4 ). Transverse or short-axis views are obtained by rotating the transducer 90 degrees counterclockwise from the long axis ( Figure 20.5 ).
Sagittal and transverse views of the bladder should be obtained for a complete evaluation of the urinary system (see Chapter 21, Bladder ).
Image Acquisition
A low-frequency transducer with deep penetration, either phased-array or curvilinear type, is used to image the kidneys. The narrower beam width of a phased-array transducer is ideal for imaging between the ribs, but the wider beam width of a curvilinear transducer allows visualization of the entire kidney longitudinally in a single view.
When scanning a patient with a suspected renal pathology, scan the unaffected side first to obtain a baseline image to compare with the affected side. To image the right kidney, place the patient in a supine position with the transducer in a coronal plane in the midaxillary to anterior axillary line at the level of the xiphoid process. Center the kidney on the screen and rotate the transducer 15-30 degrees counterclockwise to aim the transducer marker slightly posteriorly to capture a true long-axis view of the right the kidney. While holding the transducer in the same location on the skin surface, tilt or fan the transducer anteriorly and posteriorly to assess the entire kidney from its most anterior to posterior surface. Rotate the transducer 90 degrees counterclockwise from the long-axis view to obtain a transverse cross section of the kidney. Tilt or fan the transducer superiorly and inferiorly to assess the superior and inferior poles of the kidney. Figure 20.3 illustrates transducer positions to obtain long- and short-axis views of the kidney.
The left kidney is more posterior and superior than the right kidney. Placing the patient in a right lateral decubitus position facilitates visualization of the left kidney and reduces interference from the ribs and bowel gas. Requesting the patient to hold his breath in maximal inspiration will shift the kidney caudally to further reduce interference from rib shadows. Identify the left kidney with the transducer in a coronal plane on the posterior axillary line and then rotate the transducer 15-30 degrees clockwise aiming the transducer marker posteriorly to acquire a true long-axis view ( Figure 20.4 ). Transverse or short-axis views are obtained by rotating the transducer 90 degrees counterclockwise from the long axis ( Figure 20.5 ).
Sagittal and transverse views of the bladder should be obtained for a complete evaluation of the urinary system (see Chapter 21, Bladder ).
Image Interpretation
Perinephric fat and Gerota’s fascia appear as a hyperechoic stripe around the kidneys, and the fibrous capsule gives each kidney a hyperechoic outline. Normally, the renal cortex has a homogeneous appearance on ultrasound that is less echogenic than the adjacent liver or spleen. Fluid-filled medullary pyramids are seen as hypoechoic or anechoic triangular prominences in a semicircular arrangement around the sinus. As a result, the renal medulla is significantly less echogenic compared to the surrounding cortex.
The renal sinus normally appears hyperechoic due to fat content, and in the absence of urinary tract obstruction, the sinus appears homogenously hyperechoic with small anechoic pockets of urine. The ureter is usually obscured by bowel gas but may be visible with ultrasound when dilated. When distended, the ureter appears as a tubular structure extending inferiorly from the renal pelvis.
Pathologic Findings
Obstructive Uropathy and Hydronephrosis
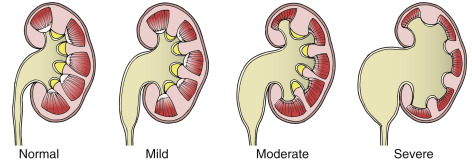
Progressively enlarging anechoic areas within the hyperechoic sinus develop with distal urinary tract obstruction and indicates hydronephrosis. The severity of hydronephrosis is classified as mild, moderate, or severe ( Figure 20.6 ) and may correlate with the size of the distal renal stone. Most algorithms incorporate the degree of hydronephrosis into a clinical decision-making pathway.