Pediatric musculoskeletal imaging was covered in a special section at the end of Chapter 8 . Congenital cardiac lesions were covered in Chapter 5 . Table 9.1 shows the appropriate imaging tests for common pediatric problems.
| Suspected Problems | Imaging Tests of Choice |
|---|---|
| Neonatal hydrocephalus or intracranial hemorrhage | Cranial US |
| Seizure | |
| Neonatal | Cranial US |
| Uncomplicated febrile seizure | No imaging needed |
| Neurologic deficit, partially unresponsive to therapy, new without obvious provoking factor | MRI without contrast |
| Posttrauma | CT head without contrast |
| Partial, generalized, intractable, or refractory seizure | MRI of head without contrast |
| Ataxia | MRI with and without contrast |
| Headache | |
| Isolated, no neurologic findings | No imaging needed |
| Isolated, with neurologic signs | CT without contrast or MRI |
| Acute “thunderclap” headache | CT without contrast |
| Migraine without neurologic signs | No imaging needed |
| Head injury | |
| Acute, mild, GCS > 13, without neurologic findings or high-risk factors | Imaging very low yield |
| Acute, mild to moderate, < 2 years of age | CT without contrast |
| Acute, penetrating, or moderate to severe | CT without contrast |
| Acute, suspected skull fracture or suspected nonaccidental trauma | CT without contrast |
| Subacute, cognitive or neurologic findings | MRI without contrast |
| Sinusitis | |
| Uncomplicated, acute | No imaging needed |
| Recurrent, unresponsive, chronic | CT of sinuses without contrast |
| Suspected orbital or intracranial complications or invasive fungal | CT with IV contrast or MRI without and with IV contrast |
| Croup or epiglottitis | Lateral soft tissue view of neck |
| Suspected inhaled foreign body | Inspiration or expiration or decubitus chest |
| Difficulty breathing | Chest x-ray |
| Fever | |
| Without obvious source, no respiratory symptoms | Chest x-ray, low yield |
| Neonatal or respiratory symptoms or increased WBC count | Chest x-ray |
| Esophageal atresia or tracheoesophageal fistula | Lateral radiograph with soft feeding tube in place |
| Asthma | |
| Uncomplicated | No imaging needed |
| Poor response to therapy, complicated | Chest x-ray |
| Suspected pneumonia | Chest x-ray |
| Congenital heart disease or congestive heart failure | Chest x-ray, echocardiogram |
| Gastroesophageal reflux (nonbilious vomiting) | Barium swallow or nuclear medicine reflux study |
| Vomiting (recurrent, 0–3 months of age) | X-ray and UGI series |
| Pyloric stenosis or new-onset, nonbilious vomiting, < 3 months of age | Ultrasound |
| Duodenal atresia or stenosis | Plain x-ray (use air as contrast) |
| Midgut volvulus | UGI series |
| Meconium ileus | Plain x-ray and meglumine diatrizoate (Gastrografin) enema |
| Appendicitis | CT with IV contrast or US (if experienced operator is available) |
| Intussusception | Plain x-ray followed by reduction using air or Gastrografin enema |
| Necrotizing enterocolitis | Plain x-ray of abdomen and possible left lateral decubitus views (to look for free air) |
| Crohn disease | CT with IV contrast or CT enterography |
| Hirschsprung disease | Barium or Gastrografin enema |
| Biliary atresia or neonatal hepatitis | Nuclear medicine hepatobiliary scan |
| Abdominal mass | Plain x-ray of abdomen and ultrasound or CT |
| Meckel diverticulum | Nuclear medicine, Meckel scan |
| Urinary tract infection (febrile and < 3 years of age or poor response to treatment) | US of kidneys and bladder |
| Hematuria | |
| Isolated (microscopic, nonpainful, nontraumatic without proteinuria) | Imaging not usually appropriate |
| Isolated (nonpainful, nontraumatic with proteinuria) | US of kidneys and bladder |
| Painful or posttrauma | CT of abdomen and pelvis without contrast |
| Rectal bleeding | See text |
| Child abuse | X-ray bone survey, CT of head without contrast, CT of abdomen if abdominal trauma |
| Back pain | |
| Uncomplicated | Imaging not appropriate |
| With constant or night pain, radicular pain, pain > 4 weeks, or neurologic signs | X ray spine area of interest; if negative, MRI of complete spine |
| Hip dysplasia (< 4 months of age) | US of hips |
| Limping (up to 5 years of age) | X-ray of affected extremity and hip; if concern for infection, US of hips and x-ray of pelvis |
| Osteomyelitis, cellulitis, or septic arthritis | Plain x-ray, MRI, or three-phase nuclear medicine bone scan |
Suspected Child Abuse
The physical examination and a history of abuse may point to obvious physical child abuse, but imaging plays a major role in detection and documentation. The injuries can involve any site but are particularly evident with fractures, as well as brain and soft tissue injuries. Fractures may be of various ages and most often involve ribs, skull, and metaphyseal and epiphyseal portions of long bones. The initial imaging workup includes an x-ray skeletal survey and computed tomography (CT) of the head without IV contrast. A CT scan of the abdomen and pelvis or chest may be needed based on the clinical examination.
Head
Imaging Techniques
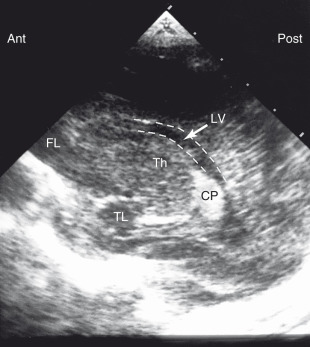
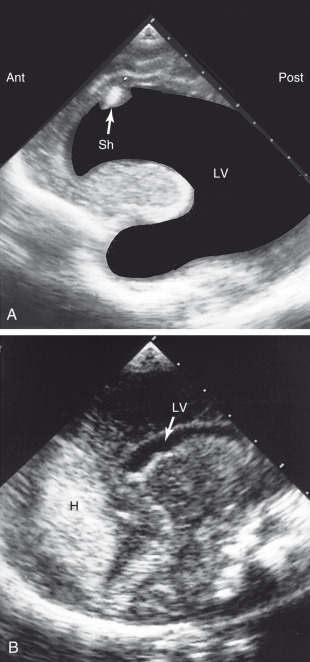
Imaging of the fetal and infant brain can be done by using ultrasound (US) as long as the fontanels remain open. Structures that can normally be visualized include the lateral ventricles, choroid plexus, thalamus, temporal lobes, and posterior fossa ( Fig. 9.1 ). The two most common indications for US of baby heads are (1) evaluation of ventricular enlargement (hydrocephalus) and (2) hemorrhage, either within the parenchyma of the brain or within the ventricles ( Fig. 9.2 ). The major advantages of US in this application are that the imaging can be done in the neonatal intensive care unit and ionizing radiation is not used. This is important, because these studies are repeated multiple times for continuing evaluation. If the fontanels are closed, CT is usually used for the evaluation of suspected hydrocephalus or hemorrhage.
Brain tumors in children are evaluated by CT or magnetic resonance imaging (MRI). With MRI, sedation is necessary, and pediatric monitoring of respiration and other functions in a very high magnetic field is difficult. CT scanning is easier to perform. About half of brain tumors in children are astrocytomas; medulloblastomas (20%), ependymomas (10%), and craniopharyngiomas (5%) are less common.
Trauma
Head trauma and the appropriate imaging studies are presented in Chapter 2 and in Table 9.1 . In general, following significant acute head trauma in a child, a noncontrast CT scan is the procedure of choice. This will reveal skull fractures and evidence of bleeding. Subacute injuries with neurologic or cognitive problems usually will have a noncontrast MRI.
Headache
Headaches are common in childhood. They may be primary (e.g., migraine, tension, cluster, exertional, cough headaches) or secondary (e.g., due to head or neck trauma, intracranial pathology, infection, thunderclap headache). MRI or CT imaging has very low yield for primary headaches but is indicated for secondary headache evaluation, especially with positive neurologic signs or increased intracranial pressure.
Childhood Seizures
Seizures may be provoked by infection, trauma, toxins, metabolic abnormality, tumor, hypoxia, cerebrovascular disease, cerebral malformation, or congenital abnormality. They also may occur without obvious cause. Neonatal seizures (usually due to hypoxic ischemic encephalopathy) typically occur in the first 7 days after birth and are evaluated with cranial US. Febrile seizures usually occur between the ages of 6 months and 4 years, and most are generalized tonic-clonic seizures. Imaging is not recommended for simple febrile seizures lasting less than 15 minutes and not recurring within 24 hours. CT or MRI may be indicated in selected patients with complex febrile seizures. Imaging is recommended for children with new-onset seizures who have experienced head trauma or partial seizures and for those who have an abnormal neurologic examination or electroencephalogram. MRI is the usual imaging modality of choice, although noncontrast CT is used initially if intracranial hemorrhage or recent trauma is suspected. For those children with a history of seizures, imaging usually is done only if the seizures are poorly controlled or are associated with a new neurologic deficit, or to follow up known abnormalities, such as a tumor.
Neck
Croup and Epiglottitis
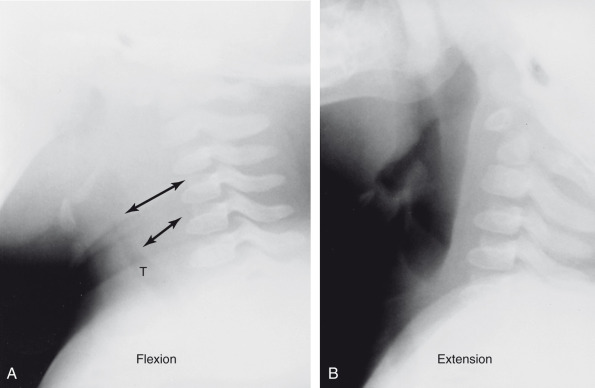
Lateral soft tissue views of the neck are often done for the evaluation of the pediatric airway. This is important in cases of suspected croup or epiglottitis. As you evaluate these lateral images, you should look to see that the child’s neck has been extended. In a young child, when the neck is flexed, the trachea can buckle forward, causing the appearance of a retropharyngeal mass. To avoid this artifact, simply extend the neck and lift the chin ( Fig. 9.3 ).
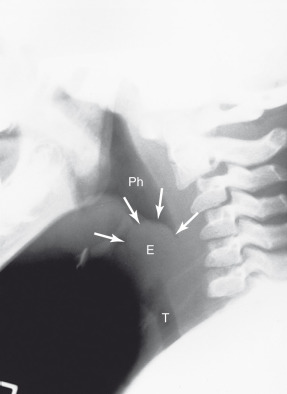
Acute epiglottitis usually occurs in older children (between the ages of 2 and 7 years) and most commonly is due to Haemophilus influenzae . This can be a life-threatening disease; the clinical findings are severe sore throat, high fever, a muffled voice, and stridor. Patients often can breathe more easily sitting up, and they drool because they cannot swallow. This is a true pediatric emergency. Because intubation can be necessary on very short notice, a physician should accompany the child to the x-ray department. The lateral soft tissue view of the neck shows a thickened epiglottis, often appearing bulbous (in the shape of a thumb; Fig. 9.4 ). Remember that the normal epiglottis is a delicate, thin, curved structure. Other findings include ballooning of the hypopharynx and subglottic edema in about one-fourth of cases.
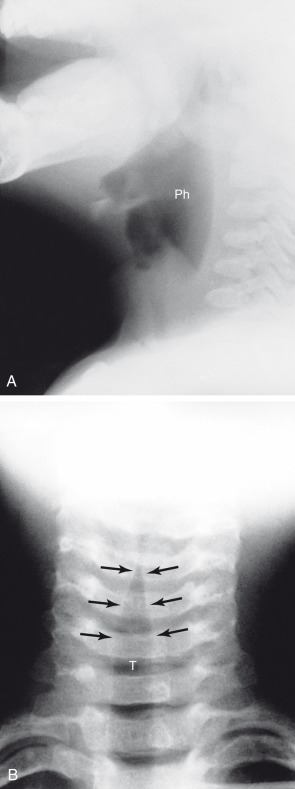
Croup typically occurs in young children (between the ages of 6 months and 3 years); it usually is caused by respiratory syncytial virus (RSV). These children often have a brassy cough (like the barking of a seal) and inspiratory stridor. Occasionally the airway may have enough edema that placement of an artificial airway is necessary. The findings on the lateral view are marked ballooning of the pharynx and hypopharynx. On the anteroposterior (AP) view, the upper portion of the trachea is shaped like a steeple ( Fig. 9.5 ). The steeple sign, caused by subglottic edema, is not pathognomonic because it also can occur in some children who have epiglottitis.
Chest
Normal Anatomy and Imaging
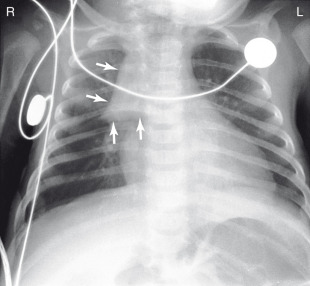
One of the major differences between the normal chest of an adult or child and a neonate is the presence of the thymus. It is routinely identified on chest x-rays from birth to approximately age 2 years. The thymus is usually seen as a widening of the soft tissues of the upper mediastinum, although occasionally it may appear to project out into the lung (known as the sail sign ; Fig. 9.6 ). Some people mistakenly think that the sail sign is an indication that a pneumothorax is present, but this is not true.
Imaging of the chest in infants and children can be difficult because of their uncooperative nature, especially when they are sick. In neonates, portable x-rays are usually obtained in the intensive care unit with the child in a supine AP projection. Somewhat older children can be placed in a holder or restrained with Velcro straps while an image is obtained. In most of these instances, the image is taken randomly with respect to inspiration and expiration. Amazingly enough, hypoinflation of the chest is usually not a problem in the interpretation of pediatric chest x-rays.
Most children with pneumonias, bronchiolitis, or reactive airway disease have hyperinflation. In most normal young children, the most superior portion of the hemidiaphragm is at the level of the posterior eighth rib. If the diaphragms are lower than this, hyperinflation should be considered, and pathology may well be present. Rotation of the patient can cause problems in interpretation. As the patient is rotated to the left, the right cardiac border projects over the spine and the right lower lobe pulmonary vessels are indistinct and can mimic an infiltrate ( Fig. 9.7 ).
A favorite x-ray examination is the so-called babygram. This is an AP view of both the chest and the abdomen. In extremely small babies, the x-ray exposure can be adequate to visualize pulmonary vasculature, bowel gas, and skeletal structures. Conversely, if you are interested only in the chest, a chest x-ray is what should be ordered to avoid unnecessary radiation exposure.
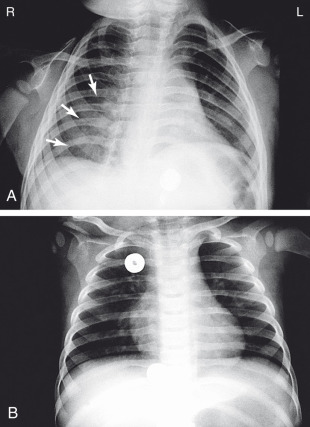
Foreign Bodies
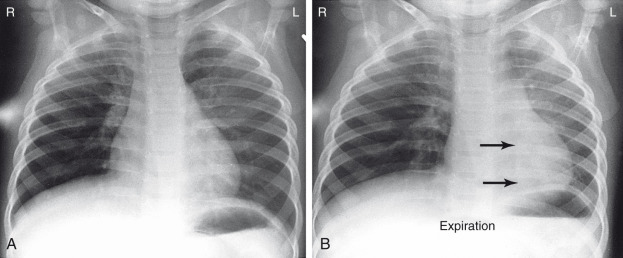
Foreign bodies can be either aspirated or ingested. Most foreign bodies consist of vegetable material (such as peanuts) or plastic. Remember that vegetable and plastic items are usually not visible on a plain x-ray. When a foreign body is aspirated into a bronchus, there are two possibilities. The first is that the object will become completely impacted and will not allow air to pass during inspiration and expiration. In this case, the air distally will become resorbed and postobstructive atelectasis or a focal infiltrate with associated volume loss will be found.
The second possibility is that the object is only incompletely obstructing the bronchus. This occurs because, during inspiration, the bronchus becomes larger in diameter and air can pass around the object. During expiration, the bronchus becomes narrower due to pressure in the lung, and the air distal to the object cannot escape. The object acts as a ball valve. Thus, if you suspect the presence of an inhaled foreign body, be sure to order inspiration and expiration images. On the inspiration image, you may see postobstructive atelectasis, or the chest x-ray may be normal. If the chest is normal, a ball valve phenomenon may still exist, and on the expiration view, air will be trapped on the affected side, whereas the unaffected lung will decrease in volume. When this happens, a resultant shift of the mediastinum toward the normal unaffected side will be seen ( Fig. 9.8 ).