A good examination in facial nerve imaging (CT or MR imaging) depends on a good knowledge of anatomy. Two clinical situations must be considered: imaging of patients with or without facial palsy. CT and MR imaging are very useful when the symptoms are atypical or progressive: MR imaging gives very good information about the facial nerve inflammation but may also discover a schwannoma, a hemangioma, a meningioma, or a primitive or secondary cholesteatoma. In malignant tumors of the parotid gland, a study of the fallopian canal must always be performed to delineate an extension in the mastoid, tympanic, or intrameatic parts. In some rare cases, a metastasis in the temporal bone may occur, especially in the region of the geniculate ganglion. Particular attention must be paid to children with facial palsy, considering the possibility of a histiocytosis or metastasis of a neuroblastoma.
The facial nerve is responsible for the motion of the face and for lacrimal, nasal, and salivary secretions. The main clinical sign that leads a clinician to ask for imaging is peripheral facial nerve palsy, which has different causes but is most frequently caused by inflammation. Both MR and computer tomography (CT) of the temporal bone are used when the facial nerve must be examined.
The following anatomic areas must be imaged when the facial nerve is studied:
The brain and pons (precentral-, postcentral-, central gyrus, posterior limb of the internal capsule)
The cerebellopontine angle (CPA)
The internal auditory canal (IAC)
The labyrinthine part of the facial nerve canal (VII-1) and geniculate ganglion (GG)
The tympanic part of the facial nerve canal (VII-2)
The mastoid part of the facial nerve canal (VII-3)
The stylomastoid foramen (SF) and the parotid gland (PG)
Technique: 1 to 1.5 Tesla
Sequences
T2 weighted, fluid attenuated inversion recovery
These images are acquired in the axial plane, perpendicular to the brainstem using a head coil. To study the brain and pons, a slice thickness of 4 mm to 5 mm and a 256 matrix is used.
T1 weighted, spin echo
T1 images are achieved parallel to the roof of the orbit using a head coil; additional surface coils centered on the ears can also be used (at 1.5 Tesla). The CPA, IAC, VII-1, GG, VII-2, VII-3 are studied on gadolinium-enhanced images, with or without fat saturation, and with a slice thickness ranging from 1 mm to 2 mm. Additional contrast enhanced T1-weighted images in the coronal plane can provide valuable information of the VII-1, VII-2, VII-3 segments of the facial nerve, and contrast enhanced sagittal T1-weighted images can be helpful in the study of VII-3.
High resolution 3-dimensional heavily T2-weighted images
Images are made in the axial plane, parallel to the roof of the orbit. Gradient echo (GE) or spin echo (SE) or fast spin-echo (FSE) sequences are used depending on the MR-unit used. These axial images have a thickness of 0.35 mm to 0.7 mm, and provide detail visualization of the nerve in the CPA, internal auditory meatus (IAM), or of the VII-1, VII-2, and VII-3 segments. Images reformatted in the coronal (VII-1, VII-2, VII-3) and para-sagittal (VII-2, VII-3) plane are very helpful in the evaluation of the different nerve segments.
T1-weighted SE images through the stylomastoid foramen and parotid gland
Axial 2-mm to 3-mm thick images parallel to the soft palate make evaluation of the facial nerve at the level of the SF and PG possible. This can be achieved using a head coil or surface coils.
Brain and Pons
Sequences: T2 and fluid attenuated inversion recovery (FLAIR)
Coils: head coil
Imaging plane: Axial, perpendicular to the brainstem
Slice thickness: 4 mm
Matrix: 256
CPA, IAM, VII-1, VII-2, VII-3: at 1.5 Tesla
T1-weighted images
Sequence: T1-weighted SE, with and without intravenous (IV) contrast administration, with or without fat saturation pulse
Coils: head coil or surface coils centered on the ears, or a combination of both
Imaging plane: axial plane, parallel to the roof of the orbit
Slice thickness: 1 mm to 2 mm, depending on the quality of the MR system
T2-weighted images
Sequence: high resolution T2-weighted GE or turbo spin-echo or FSE three-dimensional (3D) images, with IV contrast administration
Coils: head coil or surface coils centered on the ears, or a combination of both
Imaging plane:
- •
Parallel to the roof of the orbit
- •
Axial reformatted images parallel to the lateral semicircular canal for visualization of VII-2
- •
Sagittal reformatted images for visualization of the nerve in the IAC and VII-1, VII-2, and VII-3 segments of the nerve. These sagittal images, in combination with IV gadolinium administration, are very useful to identify a tumor or enhancement inside the facial canal.
Slice thickness: 0.4 mm to 0.7 mm
In case a tumor is detected
Sequence: SE T1-weighted images
Imaging plane: coronal plane with IV gadolinium administration from the GG to the VII-3 segment and in the sagittal plane for evaluation of the VII-3 segment.
Slice thickness: 1 mm to 2 mm
Stylomastoid Foramen and Parotid Gland
Sequence: SE T1-weighted image with IV gadolinium administration without fat suppression
Imaging plane: axial
Slice thickness: 2 mm to 3 mm
In summary, T2 and FLAIR sequences are used for imaging of the brain and pons (especially the motor nucleus). T1 and T2 gadolinium-enhanced high-resolution images are used to study the cerebellopontine angle and the facial nerve inside its canal in the petrous bone. For both sequences, better image quality is achieved when surface coils are used, alone or in combination with the head coil. Routine 2-mm to 3-mm thick T1-weighted SE images are used to evaluate the stylomastoid foramen and the parotid gland.
Imaging of the pathologic nerve
The most common indications for imaging of the facial nerve are as follows:
Peripheral facial nerve palsy. This is the most frequent indication. It can be caused by infectious diseases, Bell’s palsy, tumors (schwannomas or other tumors), pseudotumoral lesions, brainstem lesions, trauma, and malformations.
Tinnitus, conductive or sensorineural hearing loss, or vertigo related to a schwannoma of the facial nerve without any facial nerve palsy.
Evaluation of the facial nerve position before surgery. This is indicated before surgery in patients with otosclerosis, ossicular malformations, CPA, and IAC pathology.
Hemifacial spasm.
Evaluation of a Peripheral Facial Nerve Palsy
Nontumoral lesions of the pons with facial nerve palsy
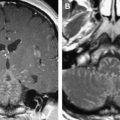
The most frequent nontumoral lesions of the brain and pons are ischemia, multiple sclerosis, hemorrhagic cavernous hemangioma, and arteriovenous malformations. They can all cause peripheral facial nerve palsy. On T2 or FLAIR images they appear as areas of hypersignal in the region of the facial nerve motor nucleus or facial nerve fibers, close to the fourth ventricle ( Figs. 1 and 2 ). Acute ischemic lesions in this region can be distinguished on diffusion weighted images (DWI) as a diffusion restriction (high signal on b-1000 images, low signal on apparent diffusion coefficient images) and, therefore, the DWI sequence should be added as a routine sequence in these patients.

Inflammation of the facial nerve
In these patients, the radiologist is asked to confirm inflammation and to eliminate a tumor. Patients most often present with Bell’s palsy without any other cranial neuropathy. The unilateral paralysis is most frequently acute and there can be associated trouble of taste or pain around the ear. The herpes simplex virus is most often causing the symptoms but cannot always be traced by laboratory tests.
In other cases, the viral origin is evident, as in the case of patients presenting with a Ramsay Hunt syndrome. Varicella-like cutaneous lesions of the external ear in association with a peripheral facial nerve palsy confirm the viral origin. Nerves V, VIII, IX, and X are then also commonly affected. There is no need for imaging in typical Bell’s palsy or Ramsay Hunt syndrome when the inflammation is clinically obvious. Imaging should be reserved for atypical Bell’s palsies, with a persistent peripheral facial nerve paralysis lasting for more than 2 months, and for recurrent or slowly progressive palsies. Imaging can also be used to confirm inflammation in anxious patients with slow or bad recovery of the facial nerve palsy.
The diagnosis of neuritis can be made in the petrous facial nerve canal (VII-1, GG, VII-2). The most interesting sequences (see above) to detect inflammation are the gadolinium enhanced T1-weighted SE and the high resolution T2-weighted sequences, such as GE constructive interference in steady state (CISS) after intravenous gadolinium injection. Viral infection can cause rupture of the blood-nerve barrier, causing edema and diffusion of gadolinium along the labyrinthine segment (VII-1) of the facial nerve ( Fig. 3 ). On axial T1-weighted SE images, this contrast material diffusion appears as a more or less important enhancement following the curvature of the labyrinthine segment of the facial nerve.
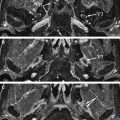
The enhancement of the tympanic and mastoid segment of the facial nerve is more difficult to delineate and evaluate. The normal veins that surround the tympanic and mastoid segment of the facial nerve in its canal take up gadolinium after IV administration as well. This results in a more or less high physiologic signal on contrast-enhanced images, which is not so easily differentiated from an abnormal condition (eg, neuritis) ( Fig. 4 ). The diffusion of gadolinium along the labyrinthine segment of the facial nerve and in the fundus of the IAC is always pathologic. High resolution SE or GE (eg, CISS) images can be used to exclude a mass or nodule in the course of the facial nerve or in the facial nerve canal. This is especially helpful in the superior upper quadrant of the IAC, where mass lesions are best excluded, or demonstrated on para-sagittal reformatted images. The facial nerve can easily be delineated in the fundus of the IAC when there is sufficient cerebrospinal fluid surrounding the nerve ( Fig. 5 ). On the other hand, if the IAC is narrow, the different nerves (facial nerve, vestibular nerves, cochlear nerve) may be squeezed together, and then it can becomes impossible to exclude a mass. Hence, it is important to analyze the IAC in detail on contrast-enhanced T1-weighted images.
Inflammation of the tympanic and mastoid segment of the facial nerve canal can be nicely demonstrated on contrast-enhanced high resolution T2-weighted images (eg, CISS GE sequence). The T1 effect of gadolinium makes it possible to depict inflammation of the tympanic and mastoid segment of the facial nerve because of the high signal intensity on these 3D high resolution T2-weighted images ( Fig. 6 ). Such a high signal is never seen inside the facial nerve canal on these images (eg, CISS) in noninflammatory cases. Therefore, there are two ways to demonstrate inflammation within the facial nerve canal: rupture of the blood-nerve barrier with abnormal gadolinium diffusion along the labyrinthine segment of the facial nerve, and high signal of the second and third segment of the facial nerve inside the facial nerve canal on the high resolution T2-weighted CISS sequence. In several cases, and especially in case of herpes simplex infection, labyrinthitis can also be present. Contrast enhancement along the superior or inferior branch of the vestibular nerve and inside the cochlea, vestibule, and semicircular canals can be seen in these patients. The perilymphatic fluid can even have a spontaneous high-signal intensity on the precontrast T1 SE images.
In summary, in most of the cases it is possible to localize the inflammation with a combination of contrast-enhanced SE T1-weighted images and high-resolution 3D T2-weighted images (CISS). However, there is no clear relation between the prognosis and the contrast enhancement. Other viruses—in case of borellia and HIV, for exmple—can also affect the facial nerve inside the facial nerve canal.
Peripheral facial nerve palsy can also occur in cases of malignant external otitis (MEO). MEO is caused by Pseudomonas aeroginosa and usually results in a localized tympanic bone infection, with a more or less important osteitis. It preferentially occurs in elderly diabetic patients. CT may nicely demonstrate the destruction of the anterior or posterior walls of the tympanic bone. Usually the inflammation spreads along the soft tissues superficial to the temporal bone and around the external auditory canal, with potential extension to the temporo-mandibular joint, the middle ear cavity, the upper part of the carotid space in the neck, the lateropharyngeal space, and more rarely the posterior or middle cranial fossa. Surgical and medical treatment may be required in patients with an associated peripheral facial nerve palsy and in whom a tumor is excluded.
Facial nerve schwannoma with facial palsy
Facial nerve schwannomas occur less frequent than eighth nerve schwannomas. Usually the lesion originates in the schwann cells with a frequent clinical sign: peripheral facial nerve palsy. However, one has to know that the peripheral facial nerve palsy is absent in 30% of the cases. Multiple schwannomas occur in patients with neurofibromatosis type II. Neurofibromas are found in type I neurofibromatosis. In these patients, additional schwannomas or neurofibromas can also be detected along the major side branches of the facial nerve, such as the greater superficial petrosal nerve and the chorda tympani. Local or more extensive enlargement of the facial nerve canal can be seen on CT. The diagnosis is easy when a mass is seen along one or several segments of the facial nerve inside the facial nerve canal. Schwannomas appear as round, well-delineated masses in the CPA, IAC, or facial nerve canal ( Fig. 7 A). They can extend to the middle ear, the stylomastoid foramen, or parotid gland. Schwannomas can also cause enlargement of the chorda tympani canal, situated between the mastoid segment of the facial nerve canal and the middle ear cavity, and this is often more subtle and more difficult to depict. The lesions can also present as a small mass in the external auditory meatus or the tympanic cavity. This “double nodule or mass” sign (tumoral lesions both in the mastoid segment of the facial nerve canal and along the chorda tympani) is typical for a nervous tumor of the facial nerve. In the middle ear, schwannomas or neurofibromas can also destroy the long process of the incus or can compress the stapes.
MR imaging is useful in the demonstration of the mass itself, from the CPA to the facial nerve canal and the parotid gland. On T1-weighted images, schwannoma have a slightly high signal intensity that can be found along the course of the facial nerve. On contrast-enhanced SE T1-weighted images, schwannomas are well delineated and strongly enhancing masses ( Fig. 7 B), with sizes ranging from several millimeters to 3 to 5 centimeters. A dumbbell appearance is classical along the facial nerve canal.
On the high-resolution T2-weighted images it is also possible to distinguish nodular masses in the CPA, the fundus of the internal auditory canal, or in the facial nerve canal ( Fig. 7 C).
Small IAC schwannomas of the facial nerve should be studied on para-sagittal reformatted images. On these images one can check if the schwannoma is localized in the anterior upper quadrant of the IAC, while the normal cochlear nerve is located in the inferior anterior quadrant and the normal vestibular nerves are located in the superior and inferior posterior quadrants. Finally, large schwannomas (several centimeters) can be very heterogeneous on MR and can have large cystic areas.
Other tumors and pseudotumors of the facial nerve
The pons
Pontine malignancies, metastatic tumors, and lymphomas may all cause peripheral facial nerve palsy. On MR, and especially on the FLAIR images, it is easier to recognize and delineate these tumors.
The CPA and IAC
Lesions occurring in these regions and which are causing peripheral facial nerve palsy are usually malignant: metastasis or lymphoma. These lesions enhance strongly on contrast-enhanced SE T1-weighted images ( Fig. 8 ). The margins are hazy and the meninges are usually thickened in case of metastasis. In lymphoma, the diagnosis can be more difficult, especially when the margins of the masses, for example in the IAC, are sharp and are therefore mimicking a neurofibroma or schwannoma. Special attention must be paid when clinical signs evolve quickly. In some cases, arachnoiditis can have the appearance of a pseudotumor; however, the thickened meninges will decreased in size under medical treatment and will heal without any scars.
The facial nerve canal
Several benign and malignant tumors or pseudotumors involve the facial nerve canal and compress the facial nerve.
Hemangioma: Based on the vascular caliber, hemangiomas are classified as capillary, cavernous or a combination of both. They are usually located in the geniculate ganglion fossa and have a short extension along the labyrinthine segment of the facial nerve canal into the IAC or along the tympanic facial nerve segment. On CT these lesions have poorly defined margins. The diagnosis is made easy if bone spiculae are present. On MR, a hemangioma can be seen as a mass in the geniculate ganglion, with intermediate signal intensity on unenhanced T1-weighted MR images. Following IV contrast administration, they enhance strongly but also become somewhat heterogeneous because of the presence of the calcified spiculae ( Fig. 9 ). Special attention must be paid to subtle extension and associated enhancement along the labyrinthine segment of the facial nerve canal. Hemangiomas are usually small, the facial nerve fibers are disorganized, and patients frequently present with facial nerve palsy. In contrast, schwannomas compress the facial nerve fibers, and in these patients often no neurologic abnormalities or clinical signs are present.
Meningioma: A meningioma may compress the facial nerve in any part of the facial nerve canal and does this most often in the geniculate ganglion fossa, causing a peripheral facial nerve palsy. Strong enhancement of the thickened meninges can be seen on axial and coronal gadolinium-enhanced T1-weighted images. The surrounding bone is heterogeneous and has irregular margins. Meningiomas can also originate in the middle cranial fossa and can then invade the Eustachian tube, the middle ear, the greater superficial petrosal nerve canal, and the geniculate ganglion fossa. Facial nerve palsy is rarely found in association with such an extension.
Secondary cholesteatoma: Secondary cholesteatoma with peripheral facial nerve palsy is rare and usually occurs after a long history of chronic otitis media. Cholesteatoma usually invades the attic superiorly, may fistule toward the labyrinth, and can compress the facial nerve in the region of the geniculate ganglion. CT can demonstrate the sequelae of chronic otitis media and is able to visualize the extension of the lesion ( Fig. 10 A). Cholesteatoma presents as a nonenhancing mass on gadolinium enhanced T1-weighted images, has an intermediate to low signal intensity on T2-weighted images ( Fig. 10 B), and has a high signal intensity on diffusion images ( Fig. 10 C). The region of the geniculate ganglion is most often involved, but the lesion can attack any part of the facial nerve canal. The cholesteatoma can also erode or invade the labyrinth and can eventually grow into the IAC.