In many respects, craniofacial trauma in children is akin to that in adults. The appearance of fractures and associated injuries is frequently similar. However, the frequencies of different types of fractures and patterns of injury in younger children vary depending on the age of the child. In addition, there are unique aspects that must be considered when imaging the posttraumatic pediatric face. Some of these are based on normal growth and development of the skull base and craniofacial structures, and others on the varying etiologies and mechanisms of craniofacial injury in children, such as injuries related to toppled furniture, nonaccidental trauma, all-terrain vehicle accidents, and impalement injuries.
Key points
- •
Mechanism of injury and growth and development of the pediatric face play a role in the type and pattern of injury in pediatric craniofacial trauma.
- •
Normal variant lucencies in the pediatric skull base are important to recognize, so as not to misdiagnose fractures.
- •
Lack of complete ossification of the anterior skull base, before the age of 4 years, should not be mistaken as a posttraumatic or congenital anomaly.
- •
Trapdoor orbital floor fractures are more common in children than adults, and can result in entrapment of orbital soft tissues, without significant displacement of fracture fragments.
- •
Beware of toppled furniture, especially the television, as a cause of significant craniofacial and skull base trauma in children.
- •
Most pediatric craniofacial impalement injuries are treated conservatively. However, imaging is very helpful to define the extent of injury and assess for retained foreign bodies.
Introduction
Craniofacial trauma in children is in many respects very similar to that in adults. The patterns of fractures and associated injuries in older children and adolescents are frequently identical to those found in adults. However, the patterns of facial injury in younger children differ from those in adults, primarily reflecting changes in anatomy and physiology of the developing face, extent of paranasal sinus pneumatization, and phase of dentition. The frequency of different types of fractures is, therefore, also variable depending on the age of the child. In addition to understanding how normal growth and development of the pediatric skull base and craniofacial structures affect the patterns of injury in children, it is important for the imager to recognize multiple normal variant lucencies in the pediatric skull base that may mimic fractures. Furthermore, a few types of injury deserve special attention in children, including injuries related to toppled furniture, nonaccidental trauma, all-terrain vehicle (ATV) accidents, and impalement injuries.
Introduction
Craniofacial trauma in children is in many respects very similar to that in adults. The patterns of fractures and associated injuries in older children and adolescents are frequently identical to those found in adults. However, the patterns of facial injury in younger children differ from those in adults, primarily reflecting changes in anatomy and physiology of the developing face, extent of paranasal sinus pneumatization, and phase of dentition. The frequency of different types of fractures is, therefore, also variable depending on the age of the child. In addition to understanding how normal growth and development of the pediatric skull base and craniofacial structures affect the patterns of injury in children, it is important for the imager to recognize multiple normal variant lucencies in the pediatric skull base that may mimic fractures. Furthermore, a few types of injury deserve special attention in children, including injuries related to toppled furniture, nonaccidental trauma, all-terrain vehicle (ATV) accidents, and impalement injuries.
Normal growth and development
Growth and development play a role in the types of craniofacial fractures that occur at differing ages. Because many of the structures are still in the process of growing and maturing, and dentition may be incomplete, pediatric maxillofacial injuries carry with them the risk of altering the function and ultimate growth of the affected structures. Therefore, timely diagnosis and prompt management are important to prevent disturbances in future growth that may affect function, dental occlusion, and cosmetic appearance. By the end of the first year of life, the mandibular halves are fused at the sypmphysis. The condyle contributes to the vertical growth of the mandible. Most growth of the zygoma and maxilla is complete by 7 years, most orbital growth is completed by 5 to 7 years of age, but cranial vault and craniofacial structures typically do not achieve growth maturity until 14 to 16 years of age. The bones of the craniofacial skeleton grow and develop by remodeling and displacement throughout young life. Remodeling occurs secondary to local factors that result in change in size and shape of each component, and displacement occurs secondary to bones moving apart at joints, sutures, and articular surfaces. The cranium and orbits grow in response to the growth of the brain and globes early during the first year of life and growth of the zygoma and maxilla is initially slower than the cranio-orbital region. Therefore, the cranio-orbital complex is larger than the maxilla-mandibular complex in infancy. Over time, the young child’s craniofacial development is altered by central nervous system, optic pathway, and speech/swallowing development and use and development of muscles of facial expression and mastication, paranasal sinus pneumatization, and normal phases of dentition. Deciduous teeth begin to erupt at approximately 6 months of age, mixed dentition is noted at about 6 years of age, and adult dentition is reached by 12 or 13 years of age.
Cranio-orbital complex is larger than the maxilla-mandibular complex in infancy
Incomplete development of the paranasal sinuses: increases stability and decreases incidence of midface fractures
Incomplete dentition: increases stability and decreases incidence of mandible fractures, rare in infants
Normal variant lucencies in the skull base
The postnatal development of the anterior and central skull base is complex, and beyond the scope of this article. The central skull base (chondrocranium) is composed of at least 25 separate ossification centers in the embryo that ultimately contribute to the mature sphenoid and occipital bones. Throughout childhood, there are many normal skull base sutures, fissures, synchondroses, vascular channels, and clefts that can routinely be identified on head and neck computed tomography (CT) imaging in children. Knowledge of the normal developmental anatomy of the skull base is important to prevent misinterpretation of these findings as fractures, osseous lesions, and cephaloceles.
A large number of normal lucencies are identified in the central skull base, including but not limited to the spheno-occipital synchondrosis, olivary eminence, craniopharyngeal canal, canalis basilaris medianus, median raphe of the basiocciput, and coronal clefts of the basiocciput. In addition, there are normal variant lucencies in the occiput that should not be confused with fractures. These include remnants of the anterior intraocciptial synchondrosis, and posterior lucencies related to variant fusion of Kerckring ossicle.
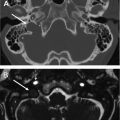
At birth, there are multiple separate ossification centers that ultimately form the mature sphenoid bone, all of which are initially separated from the adjacent centers by a nonossified synchondrosis. The most commonly visualized synchondrosis related to the sphenoid bone on postnatal CT is the spheno-occipital synchondrosis. Most skull base growth occurs at the spheno-occipital synchondrosis, which separates the postsphenoid ossification center from the basiocciput and remains patent until teenage years ( Fig. 1 ). During closure, small ossified bodies may be identifiable within the spheno-occipital synchondrosis ( Fig. 2 ). After closure is complete, there are frequently small divots, clefts, or fissures on one or both sides of the spheno-occipital synchondrosis.
In infants, the sphenoid body frequently contains two visible midline foramina, an anterior triangular-shaped lucency and a round posterior foramen. The anterior cartilage-containing structure is called the olivary eminence ( Fig. 3 ) and is not identifiable in most older children, but may be visible as a sclerotic remnant in 11.2% of children older than 9 months of age. The round posterior foramen, the craniopharyngeal canal, is a tubular lucency extending from the floor of the sella turcica to the roof of the nasopharynx ( Fig. 4 ). The craniopharyngeal canal is visible on CT in 8.5% of children, and as a partial canal or sclerotic remnant in 20% of children. Rarely, this canal is pathologically widened secondary to the presence of cephaloceles that frequently contain ectopic adenohypophysis ( Fig. 5 ).
Most normal-variant lucencies in the occipital bone involve the basiocciput or the region of the Kerckring ossicle. Occasionally, midline lucency in the basiocciput, called the canalis basilaris medianus, is identified posterior to the spheno-occipital synchondrosis ( Fig. 6 ). This structure may be variable in shape, and complete or incomplete. The canalis basilaris medianus is thought to represent a remnant of the cephalic end of the notochordal canal, most frequently is an incidental finding, but is rarely associated with nasopharyngeal cysts ( Fig. 7 ). The anterior intraoccipital synchondrosis has a variable appearance over time, and during fusion may progress from a somewhat cross-shaped appearance to a small well-corticated round lucency ( Fig. 8 ). Coronal clefts involving the basiocciput may also occur. Finally, lucencies related to variant fusion of Kerckring ossicle include unfused and partially fused Kerckring ossicles ( Fig. 9 ), both of which, if not recognized as normal variants, may be misinterpreted as fracture. When fracture is suspected on axial imaging, three-dimensional reconstructions in these children are frequently very helpful to better define the lucencies as normal variants related to Kerckring ossicle rather than fracture lines. Three-dimensional reconstructions are also helpful in proving that lucencies related to intrasutural bones, when they occur anywhere in the skull, are not fractures.
Spheno-occipital synchondrosis: may see remnant clefts, fissures, or small ossified bodies
Olivary eminence: only identifiable in infants
Craniopharyngeal canal: floor of sella to roof of nasopharynx, completely fuses in most children, rarely contains cephalocele
Canalis basilaris medianus: usually incidental finding, rarely associated with nasopharyngeal cysts
Median raphe of the basiocciput
Coronal clefts of the basiocciput
Anterior intraocciptial synchondrosis: changes shape over time from somewhat cross-shaped to well-corticated round lucency
Unfused or partially fused Kerckring ossicle: may be confused with fracture
Normal anterior skull base ossification
Imagers must also recognize several additional potential pitfalls related to the complex ossification pattern of the anterior skull base in order not to mistake such items as incomplete or multiple ossification centers as a defect from trauma, or as a cephalocele. Anterior skull base ossification occurs in a fairly predictable fashion, but with varying rates in young children. Most of the skull base at birth is composed of cartilage ( Fig. 10 ). During the first few months of life, there is progressive ossification of the cribriform plate, roof of the nasal cavities, and crista calli. Ossification of the cribriform plate begins near the region where the superior and middle turbinates attach and extends medially to reach the crista galli by about 2 months of age. Ossification extends from the cribriform plate, and proceeds posteriorly more quickly than anteriorly, therefore a nonossified gap is frequently present anterior to the crista galli in very young children. Only 4% of children in a study by Hughes and colleagues had complete ossification of the anterior skull base by 2 years of age, whereas all patients had a fully ossified anterior skull base by the age of 3 years, 10 months ( Fig. 11 ). After 4 years of age, the only unossified normal structure that remains in the midline anterior cranial fossa is the foramen cecum, just anterior to the crista galli ( Fig. 12 ), which may transmit a small vein.
Majority is unossified at birth
4% of children have completely ossified anterior skull base by 2 years of age
All children fully ossified anterior skull base by 4 years of age
After 4 years, only unossified portion of anterior skull basea is foramen cecum
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


