Anatomical organ
Comments
Wide pelvis
Appears to contribute to the increased risk of injury to the hip and the outer aspect of the knee, leg, and foot because of the varus tilt
Femoral anteversion and high degree of external rotation of the hip
Athletes with greater passive external rotation of the hip joint had a higher incidence of tibial stress fractures than those with lower extent of rotation
Genu varum and genu valgum
Narrow tibia and short tibial lengths
Predispose for tibial fracture
Leg dominance
However, stress fractures were more likely to occur in the dominant limb
Leg-length discrepancy (e.g., >0.5 cm.)
Friberg (1982) found that tibial, metatarsal, and femoral stress fractures were more likely to occur in longer limbs, and fibular fractures were more likely to occur in shorter limbs
Foot arch height
Flat feet
Overpronate
Malleolar torsion and range of subtalar joint motion flexibility
Muscles
Ligament
Forces
Bending forces
In a biomechanical analysis of the pathogenesis of tibial stress fractures in military recruits, Milgrom et al. (1988) concluded that bending is the most important force involved in their development, rather than torsion, tensile, and compressive forces
41.4.2 Hormonal and Body Habitus
41.4.2.1 Osteoporosis and Low BMD
Low bone mineral density (BMD) values predispose an individual to those fractures caused by compressive loads, such as those seen in the vertebrae of postmenopausal, osteoporotic women (Giladi et al. 1991; Speed 1998; Davis et al. 1990). It was suggested that athletes with osteoporosis are more likely to have fractures (Barrow and Saha 1988; Bennell et al. 1995; Myburgh et al. 1990); others did not find this correlation (Giladi et al. 1991). However, no relationship has been found between BMD and tibial stress fractures (Giladi et al. 1991; Speed 1998; Greene 1999).
41.4.2.2 Menstrual Irregularity
A history of amenorrhea and menstrual irregularity, are risk factors for injuries (Shaffer et al. 2006). The longer the duration of amenorrhea, the more likely female athletes suffer from injury (Bennell and Brukner 1997; Greene 1999; Knobloch et al. 2007; Shaffer et al. 2006; Davis et al. 1990; Barrow and Saha 1988; Myburgh et al. 1990). It was found in one study that incidence of fracture is inversely proportional with the number of menses per year (Jones et al. 2002; Knobloch et al. 2007; Barrow and Saha 1988; Edwards et al. 2005; Bennell et al. 1995). Females with “female athlete triad” (Greene 1999; Shaffer et al. 2006; Knobloch et al. 2007; Shangold et al. 1990; Hoch et al. 2009; Nattiv et al. 2007; Torstveit et al. 2005; Hobart and Smucker 2000) have a higher incidence of stress fractures (45 % compared with 29 % of runners with normal menstrual cycles).
Female runners who were taking oral contraceptives were half as likely to get stress fractures over the course of a year as those who were not taking oral contraceptives (Jones et al. 2002; Knobloch et al. 2007). Other investigators did not support this theory (Bennell et al. 1995; Myburgh et al. 1990).
41.4.2.3 Low Body Mass Index (BMI)
41.4.2.4 Eating Disorders
Athletes with eating disorders and weight fluctuations participating in sports, in which leanness is emphasized, have an increased incidence of stress fractures (Speed 1998; Greene 1999; Barrow and Saha 1988; Edwards et al. 2005; Bennell et al. 1995). It has been previously demonstrated that dietary calcium intakes more than 800 mg/day may be protective against stress fracture in athletes (Myburgh et al. 1990). Risk of stress fracture was not associated with current calcium intake by other studies (Bennell et al. 1995).
41.4.3 Demographic Characteristics
41.4.3.1 Age
An athlete with a developing skeleton is more susceptible to musculoskeletal injuries (Speed 1998). Although some studies have found a younger age to be a possible risk factor for musculoskeletal injuries, others have found older age increases the risk of injuries (Jones et al. 2002; Gall et al. 2008; McBryde 1985; Winfield et al. 1997; Peterson et al. 2000).
41.4.3.2 Race
White and Asian women have increased risk of fractures compared to black women. In one study it was found that Hispanic women were almost twice as likely to incur a stress fracture as black women. Lowest rates of stress fractures are among black women (Jones et al. 2002; Giladi et al. 1991; Speed 1998; McBryde 1985; Brudvig et al. 1983).
41.4.3.3 Height
41.4.3.4 A History Musculoskeletal Injury
History of previous injury (Gall et al. 2008; Alonso et al. 2010) is considered as a risk factor for musculoskeletal injury by some authors; other studies from the military studies did not find a relationship between prior injury and the risk of stress fracture during basic training (Jones et al. 2002; Bennell et al. 1995; Chang and Harris 1996; Ross and Woodward 1994; Shaffer et al. 1999).
41.4.3.5 Military Recruits (Speed 1998; Chang and Harris 1996; Shaffer et al. 2006)
A major factor in the development of injuries in this group is believed to be the rapid onset of training which did not allow for a progressive exposure to stress and the development of tolerance.
41.4.3.6 Personality (Speed 1998)
Another factor contributing to injuries in women may be their inability to differentiate between pushing themselves beyond the pain threshold and exposing themselves to undue risk of injury (Gall et al. 2008; Kowal 1980; Edwards et al. 2005; Clanton and Solcher 1994; Pell et al. 2004; Verma and Sherman 2001).
41.4.4 Mechanical Strain Environment
Weather
Footwear: army boot has proved quite satisfactory for men during basic training; women report that the heel width is too great even in the narrow sizes used by them. This is further aggravated by the apparent lack of heel stability inherent in the army boot used by the women during basic training. The resulting heel instability aggravates existent ankle weakness or foot disorder. Non-fitted shoes lead to foot and ankle pain and injuries, and high heels often lead to hammer toe, ingrown nails, sesamoid injuries, Morton’s neuroma, back pain, and other problems (Speed 1998; Clanton and Solcher 1994; Pell et al. 2004; Verma and Sherman 2001).
41.4.5 Activity Related
41.4.5.1 Type of Sports
All activities are not equal in the risk and sites of stress fracture. Ten percent of running injuries seen in sports injuries clinic are stress fractures (Brukner et al. 1996), particularly affecting the tibia, fibula, and metatarsals (Angus and McBryd 1976; Giladi et al. 1985; Blair and Hanley 1980). Basketball, gymnastics (pars interarticularis), and aerobic dance (e.g., tibial shaft) are also frequently involved (Speed 1998; Field et al. 2011). Upper limb stress fractures are relatively rare but are particularly seen in repetitive throwing activities (Speed 1998). Stress fractures of the pubic rami seem to be particularly common among long-distance running athletes. Military studies indicate that different types of units and different types of training may place military personnel at different degrees of risk (Jones et al. 2002).
41.4.5.2 Aerobic Fitness and the Rate of the Loading
Aerobic fitness and the rate of the loading applied to the limb appear to have an important effect on the potential for the subsequent development of a stress fracture. Low levels of aerobic fitness before recruit training have been consistently identified as a risk factor among women in the military (Giladi et al. 1991; Speed 1998; Shaffer et al. 2006; Bell et al. 2000; Jones et al. 1993; Winfield et al. 1997). Women who rated their current fitness as fair or poor were twice as likely to incur a stress fracture as were women who rated their current fitness as excellent or very good (Jones et al. 2002; Giladi et al. 1991; Speed 1998; Kowal 1980; Edwards et al. 2005; Clanton and Solcher 1994; Pell et al. 2004; Verma and Sherman 2001).
Other factors have been suggested including:
Mismatch between strength and skill and lack of previous experience (Jones et al. 2002; Gall et al. 2008).
Competitive sports and level of competition (Jones et al. 2002; Gall et al. 2008; Giladi et al. 1991).
Inadequate recovery/rest periods and training with fatigued muscle (Kowal 1980).
Continued hard training after onset of symptoms (Kowal 1980).
Intensity of exercise (Jones et al. 2002; Gall et al. 2008; Giladi et al. 1991; Edwards et al. 2005; Bennell et al. 1995; Myburgh et al. 1990), mileage (Jones et al. 2002; Harrast and Colonno 2010), and number of training cycles (Edwards et al. 2008; Lappe et al. 2001); the risks of musculoskeletal problems associated with high-intensity physical activity exceed those associated with moderate physical activity.
Training errors, training regimen (Gall et al. 2008; Speed 1998; Clanton and Solcher 1994), and lack of supervision.
Equipment failure and weather condition (Alonso et al. 2010).
41.5 Common Injuries in Female Athletes
The type and site of female injuries varies widely with type of the sport. Some sports are associated with high rate of injuries with variable site and severity (Jones et al. 2002; Gall et al. 2008; Speed 1998; Alonso et al. 2010). Any part of the body can be affected. In girls, most injuries are caused by playground activities, basketball, cycling, and general exercise (Gall et al. 2008; Knobloch et al. 2007; Freeman and Corley 2003). The most frequent diagnoses include strains/sprains followed by fractures. Many authors reported the lower limb as the commonest site for female athletic injuries (Gall et al. 2008; Engström et al. 1991; Giza et al. 2005; Jacobson and Tegner 2007), but still there were some difference in the distribution of these injuries in the lower limb (Gall et al. 2008; Kowal 1980).
41.5.1 Head Injuries
Although sports injuries contribute to fatalities infrequently, the leading cause of death from sports-related injuries is traumatic brain injury (TBI). Many sports have been associated with a variety of neurological injuries affecting the central nervous system (CNS), with some injuries specific to that sport (Gall et al. 2008; Alonso et al. 2010; Lindsay et al. 1980; McCrory et al. 2009; Collie et al. 2001; Hinton-Bayre et al. 1999; Toth et al. 2005). TBI can be seen in basketball, water sports, soccer, gymnastics, dance, and cheerleading (Gall et al. 2008; Morris et al. 1980; Toth et al. 2005; Boden et al. 2003; Noguchi 1994; Mueller and Cantu 1990). Women who participate in sports such as scuba diving or high-altitude climbing are at risk of brain injury through other mechanisms of brain damage (ischemia, nitrogen narcosis, and hypoxia) (Fothergill et al. 1991; Regard et al. 1989). The National Collegiate Athletic Association Injury (NCAA) Surveillance System between 1997 and 2000 indicated that female college athletes experience a greater number of concussions during games than male college athletes (Broshek et al. 2005; Covassin et al. 2003). Some authors report that women appear to have a greater likelihood of post-concussion syndrome at the 1-month follow-up, a greater incidence of depression following mild TBI, and a greater number of persisting symptoms 1 year after mild brain injury (Broshek et al. 2005; Bazarian et al. 1999; Rutherford et al. 1979). Younger players were more at risk for concussion than older one (Gall et al. 2008). According to cheerleading data from the United States (Consumer Product Safety Commission (CPSC) in the United States) in 2007, head and neck injuries accounted for 15.1 % of total cheerleading injuries (Broshek et al. 2005).
Head injury can result in brain concussions, contusions, skull fractures, and internal injuries, coma, and death. Brain imaging includes computerized axial tomography (CT scan) and magnetic resonance imaging (MRI) (Lindsay et al. 1980).
41.5.2 Spinal Injuries
One of the most catastrophic injuries in sports is spinal injury (Silver 1993). Spinal injuries are less common in women than men, and this could be either as a result of more aggressive behavior or a higher degree of competitiveness or possibly because the disciplines are different – women’s gymnastics emphasizes agility, grace, and dance, whereas men’s is more dependent on strength (Silver 1993).
Repetitive bending and twisting put athletes at risk for spinal injuries. The lumbar vertebrae are more prone to injury especially during sports participation. Neck muscle strains, ligament sprains, and disk and vertebral injuries are common (Silver 1993). Difficult maneuvers involving “flight” account for most spinal injuries. During these activities, the athlete is airborne and lands on a hard surface, such as the floor in gymnastics or the water in diving maneuvers. Spondylolysis and spondylolisthesis can result from repetitive hyperextension of the lower back, such as excessive back bends by gymnasts (Silver 1993; Kruse and Lemmen 2009). Disk herniation most commonly results from repetitive trauma to the back from heavy lifting or from participation in sports that require very strenuous training, such as gymnastics. Fractures can result from a blow to the back and certain parts of the vertebrae. Activities in which the athlete can get hit in the back or can fall from a great height can lead to spinal fractures (Silver 1993). Women participating in gymnastics and horse riding might be affected with spinal injury (Silver 1993; Kruse and Lemmen 2009).
Plain radiographs with multiple views should be performed. Those patients who are symptomatic despite a normal plain radiograph require further investigation in the form of a bone scan, single-photon emission computed tomography (SPECT) scan, or magnetic resonance imaging.
41.5.3 Shoulder Injuries
Shoulder injury happens frequently in sports because overuse, collision, or a fall can be the source. While tennis, baseball, swimming, and football generate many of these incidents, accidental shoulder trauma can occur in relation to nearly any athletic activity (Gall et al. 2008; Alonso et al. 2010). Common injuries include muscle strains and tears of the rotator cuff tissue or tendinopathy and shoulder fractures and dislocation. Overuse problems can be perceived as pain, shoulder instability, and scapular dysfunction, which in many cases will influence an athlete’s performance (Myklebust et al. 2011; Bahr 2009; Fahlström and Söderman 2007).
An acute dislocation of the shoulder is an extremely painful injury. It usually occurs as a result of a fall onto an outstretched hand. Traumatic anterior shoulder dislocation injuries have shown high incidents of the sudden tearing of the labrum and ligaments from the bone of the socket (Gall et al. 2008; Alonso et al. 2010). This type of injury is common in snowboarders and skiers and might be associated with fracture-dislocation of the glenohumeral joint.
The clavicle is the commonest site of fracture of the shoulder joint. Shoulder injury to the clavicle occurs in contact sports, such as football, or may result from the transmission of force in a fall up the arm or due to landing on a shoulder, or receiving a blow to the collarbone itself during a fall can also result in a fracture. The most common site of fracture is at the junction of the middle and outer third (Gall et al. 2008; Alonso et al. 2010).
Rotator cuff injuries represent shoulder injury to the muscles and tendons of the rotator cuff. Tendon and muscle strain to the rotator cuff may be most well known among baseball pitchers, tennis players, and swimmers (Jobe et al. 1989; Gomoll et al. 2004; Holtby and Razmjou 2004). Impingement syndrome is also known as thrower’s shoulder due to the prevalence of the condition among athletes who compete in throwing events. Impingement syndrome is often caused by rotator cuff tendinitis and occurs when the swollen tendons become trapped in the subacromial space. This injury is commonly caused by overuse; in this instance it is caused by the repeated throwing action (Gohlke et al. 1993; Barr 2004).
Acromioclavicular joint (ACJ) sprains usually result from a fall with direct impact on the outside of the upper arm and may lead to damaged and tearing to this ligament, causing subluxation or complete dislocation (Gall et al. 2008; Alonso et al. 2010).
41.5.4 Elbow Injuries
Athletic injuries of the elbow are common especially in throwing sports such as baseball and tennis (Frostick et al. 1999). Most injuries in the athlete are chronic overuse injuries (Alonso et al. 2010) as a result of repetitive overload resulting in micro-tears of the soft tissues. Elbow injuries are typically seen in baseball players and tennis players because of repetitive throwing or swinging motions and can be seen in gymnasts and swimmers (Frostick et al. 1999).
Tennis elbow, or lateral epicondylitis, is the general term for an overuse injury to the extensor muscles of the forearm. When these tendons become inflamed, it causes pain on the outside of the elbow. This injury occurs from excessive flexion or rotation of the elbow, and pain is located on the inside of the elbow (Frostick et al. 1999; Maylack 1988; Nirschl 1986; Stockard 2001).
The elbow is susceptible to sprains while playing certain sports. Elbow hyperextension sprains occur when the elbow is forcibly straightened past its normal range of motion, and this type of sprain happens most frequently in contact sports and in martial arts (Frostick et al. 1999).
Elbow dislocations occur when either the radius or ulna or both are forced out of the joint capsule. Most elbow dislocations occur posteriorly. A hard fall on an outstretched hand while the elbow is flexing and twisting can cause this type of injury (Frostick et al. 1999).
Tendinopathy or inflammation of the muscle that attaches to the bone of both the triceps and biceps tendons leads to pain at the elbow joint. Posterior elbow pain that worsens with elbow extension is associated with triceps tendinopathy, while anterior elbow pain that worsens with repeated elbow flexion may indicate biceps tendinopathy. Sports which involve repetitive hyperextension of the elbow, such as tennis, can lead to posterior impingement (Frostick et al. 1999; Maylack 1988; Nirschl 1986; Stockard 2001).
41.5.5 Wrist
Wrist injuries are common in athletes. They may result from a single, traumatic force or are a result of repetitive loading activity and more common in younger age group.
Three percent to 9 % of all athletic injuries involve the hand and wrist (Peters and Eathorne 2005; Rettig 2003). This number is as high as 46–87 % of gymnasts suffering wrist injuries (Manusov 2002; De Smet et al. 1994; Webb and Rettig 2008).
Injuries of the wrist can be divided into acute traumatic injuries and overuse injuries.
Acute wrist fractures are common injuries among athletes (Peters and Eathorne 2005). Distal radius metaphyseal and physeal fractures are common in skating, football, basketball, and snowboarding. The scaphoid is the most commonly injured carpal bone, accounting for 70 % of carpal fractures (Rettig and Patel 1995). An athlete falling on an outstretched hand with the wrist dorsiflexed is a common mechanism (Webb and Rettig 2008).
Reportedly, up to 87 % of elite gymnasts sustain distal radial physeal injuries (Manusov 2002). Stress fractures occur in athletes whose sports requires repetitive motion involving wrist compression or twisting as gymnastics (Webb and Rettig 2008).
Hook of hamate fractures have been seen in baseball, golf, and tennis players from the repetitive stress of the bat, club, or racquet, respectively (Webb and Rettig 2008; Stark et al. 1977). Repetitive stress is also thought to be a cause of avascular necrosis of the lunate or Kienböck’s disease (Stark et al. 1977; Mirabello et al. 1992).
Soft tissue injuries may either be due to acute trauma or overuse. Overuse syndromes such involving many tendons around the wrist are also common (Mirabello et al. 1992). Carpal dislocation typically requires significant force, such as a fall from a height in cheerleading (Peters and Eathorne 2005; Webb and Rettig 2008).
Radiographic examination is routinely used in the initial evaluation of a suspected acute wrist fracture (Russin et al. 2003). However, because of overlapping structures, many fractures are not found at initial radiographic examination (Welling et al. 2008). Radiography has 70–80 % sensitivity for detecting wrist fractures (Welling et al. 2008). Because of this, other imaging methods such as bone isotope scan and CT are also used both in the primary evaluation of suspected wrist fractures and in the assessment of bone healing after fracture (Kiuru et al. 2004; Metz and Gilula 1993).
41.5.6 Thoracic Injuries
Chest injuries in contact and collision sports are relatively rare, particularly those that are life-threatening. These injuries mostly occur with blunt trauma to the chest/thorax (Amaral 1997; Scott and Scott 1993).
Potential life-threatening injuries and conditions that may be encountered include flail chest, open chest wounds, pneumothorax, tension pneumothorax, hemothorax, myocardial contusion, cardiac tamponade, and diaphragmatic rupture. Each of these conditions is a possible occurrence in injuries sustained while participating in collision/contact sports (Gregory et al. 2002; Scott and Scott 1993).
Stress fracture is most likely to occur in the first rib (Gregory et al. 2002; Scott and Scott 1993). Overhead athletes such as basketball or tennis players are typically at risk here. Acute rib fractures are the result of direct injury. Fractures of the first and second ribs suggest a very significant transfer of energy and can be associated with underlying injuries to the thoracic aorta. Fractures are easily overlooked on a chest X-ray but are useful to detect associated abnormality like pneumothorax. Bone isotope scan is helpful in detecting occult fractures in the ribs (Gregory et al. 2002; Scott and Scott 1993). Fracture of the costal cartilage is a rare cause of chest pain in athletes. Cross-sectional techniques such as CT, sonography, and MRI have been shown to be useful in muscle and soft tissue injury and more sensitive than radiography (Griffith et al. 1999; Miller 2006; Malghem et al. 2001).
Sternal fractures are the result of direct high-energy trauma and rare in sports. Sternoclavicular dislocation usually results from a fall or blow to the front of the shoulder or a fall onto an outstretched hand.
41.5.7 Hip and Pelvis Injuries
The most common injuries of the hip and groin region in athletes are myotendinous strain injuries. They occur when a muscle is stretched beyond a tolerable length causing it to tear (Palmer et al. 1999; Marcantonio and Cho 2000). The most common location for a muscular strain to occur is where the muscle attaches to its tendon; they can also occur within the muscle belly themselves (Jones et al. 2002; Alonso et al. 2010; Marcantonio and Cho 2000; Brittenden and Robinson 2005).
Avulsion fractures of the apophyses and spines of the pelvis are usually considered uncommon injuries, seen almost exclusively in adolescent athletes mainly as a result of the sudden, forceful, or unbalanced contraction of the attached musculotendinous unit in sporting events such as kicking a ball, running, or jumping (Knobloch et al. 2007; Tehranzadeh 1987; Kujala and Orava 1993; Veselko and Smrkoly 1994; Fernbach and Wilkinson 1981; Metzmaker and Pappas 1985). This lesion is observed in soccer players and observed in women’s gymnastics. For example, injuries to the ischial tuberosity are seen in gymnastics (Tehranzadeh 1987; Kujala and Orava 1993; Veselko and Smrkoly 1994; Fernbach and Wilkinson 1981; Metzmaker and Pappas 1985). Inflammation of the bursa outside the hip joint, the so-called trochanteric bursitis, can cause pain with hip movement. The labrum can be torn by a twisting or slipping injury or over time by repetitively compressing the labrum between the femoral head and cup (Fernbach and Wilkinson 1981).
Osteitis pubis is thought to be due to the repetitive pull of muscles over the front of the hip joint. Usually pain is activity related and often seen in runners, soccer players, and hockey players. Complete dislocation of the hip joint is a very unusual, but subluxation is more common and might result in avascular necrosis of the hip (Brittenden and Robinson 2005; Kujala and Orava 1993).
A hip pointer is a bruise to the iliac crest of the pelvis. Hip pointers occur from a direct blow to the iliac crest. Because of the superficial location of the iliac crest, it is very susceptible to impact injuries. Hip pointers frequently occur during football but can occur in any sport where the iliac crest is at risk to direct impact (Brittenden and Robinson 2005).
Stress fractures of the hip are usually seen in long-distance runners (Knobloch et al. 2007) and much more common in women than in men (Major and Helms 2000; Spitz and Newberg 2002; Deutsch et al. 1997). The muscles and soft tissues of the pelvis protect the skeleton from the effects of repeated stress explaining the greater incidence of pelvic stress fracture in female athletes, with their relatively reduced muscle bulk. They are more common in sports that involve jumping and landing on hard surfaces, such as distance running, ballet, basketball, and gymnasts. Running athletes are most commonly affected with the femoral neck and the inferior pubic ramus most frequently involved although sacral fractures (Knobloch et al. 2007; Johnson et al. 2001) are not unknown (Veselko and Smrkoly 1994; Major and Helms 2000).
41.5.8 Knee Injuries
Injuries to athlete knees can result from contact or noncontact injuries.
Athletes in all different sports are susceptible to overuse injuries in the knee, primarily due to repetitive movements such as jumping, cutting, and sudden starts and stops. Soccer, ice hockey, volleyball, basketball, alpine skiing, and judo are the sports with a high proportion of knee injuries (Gall et al. 2008; Backx et al. 1991). There is growing evidence on the higher vulnerability of the knee in females (Gall et al. 2008; Alonso et al. 2010; Arendt and Dick 1995; de Loe et al. 2000). Ligament injuries to the knee are very common in sports that require stopping and starting or quickly changing directions. These extreme forces on the knee can result in torn ligaments (Gall et al. 2008). The anterior cruciate ligament (Gall et al. 2008) and the medial collateral ligament are the most often injured, but the posterior cruciate ligament and the lateral collateral ligament can also be injured. The anterior cruciate ligament injuries usually affect female more than male (Wojtys et al. 1998; Dugan 2005; Arendt and Dick 1995; Backx et al. 1991).
Cartilaginous injury usually affects either the medial meniscus or lateral meniscus. Meniscus tears are often the result of twisting, pivoting, decelerating, or a sudden impact.
Osteoarthritis is another cause of knee pain in athletes and results in a gradual loss of joint cartilage due to prolonged repetitive trauma (Niva et al. 2006). Jumper’s knee, also known as patellar tendinopathy, refers to damage of the patellar tendon which connects the knee cap to the tibia.
Complete dislocation of the knee is an uncommon trauma. Because of the potentially severe neurovascular damage, knee dislocation can be limb threatening (Peltola et al. 2009; Robertson et al. 2006).
Stress fracture is common around the knee and can affect either the lower femur, upper tibia, or patella especially if the latter is weakened by osteoporosis or chondromalacia (Edwards et al. 2005; Niva et al. 2006; Mason et al. 1996).
Iliotibial band syndrome is another cause of pain around the knee (ITB syndrome). The iliotibial band runs from the pelvis to the knee and serves to protect and support the knee joint. ITB syndrome occurs when the band repeatedly rubs against the lateral femoral condoyle; it consequently becomes irritated and inflamed; this is usually due to overuse. Iliotibial band syndrome is also a common injury found among female runners and triathletes (Edwards et al. 2005).
Chronic exertional compartment syndrome of the lower leg generally is induced by exercise that impairs neuromuscular function within the involved compartment. In young athletes, it often presents in bilateral form, with equal incidence in male and female athletes. Nerve entrapment and popliteal artery entrapment syndrome are other causes of lower leg pain in athletes (Edwards et al. 2005; Clanton and Solcher 1994; Styf 1988; Touliopolous and Hershman 1999).
41.5.9 Tibia
Although complete fracture of the tibia might happen in case of severe contact trauma, the tibia is a common site of noncontact overuse stress fracture (Boden et al. 2000).
A very common overuse injury affecting players of all sports is the medial tibial stress syndrome (MTSS) or what is called shin splints. Shin splints result from inflammation of the tissues surrounding the tibia (Edwards et al. 2005). This is caused by a number of factors such as a rapid increase in training, poor flexibility, or repetitive contact (jumping or running) on hard surfaces. Stress fracture of the fibula is less common but was described by some authors (Angus and McBryd 1976; Edwards et al. 2005; McBryde 1985; Blair and Hanley 1980; Brukner et al. 1996).
41.5.10 Ankle Injuries
The most common of all athletic injuries are ankle injuries, ranging from 17 to 20 % of injuries in most sports (Gall et al. 2008; Alonso et al. 2010; Toth et al. 2005; Bahr and Reeser 2003). Ankle sprains are the most common foot and ankle injuries seen in athletes (Gall et al. 2008; Alonso et al. 2010; McKeon Pk and Mattacola 2008). Muscle weakness and muscle imbalances have been implicated in persistent ankle pain and recurrent ankle sprains. The lateral ligaments are most commonly injured (Jobe et al. 1989; Gohlke et al. 1993).
Osteochondral lesion of the talus is defined as the separation of a fragment of the articular cartilage, with or without subchondral bone (Myklebust et al. 2011; Bahr 2009). The misdiagnosis or delayed diagnosis of osteochondral lesions of the talus occurs in up 81 % of patients presenting with chronic ankle pain (Toth et al. 2005; McKeon Pk and Mattacola 2008).
Achilles tendinosis is caused by repeated micro-tears to the Achilles tendon, leading to damage and loss of healthy tissue. Achilles tendinitis can progress either rapidly over a couple of days or gradually over several months (Cook and Purdam; continuum tendinopathy BJSM 2009). Usually the area 4–6 cm proximal to the calcaneus is especially predisposed to tendinopathy and subsequent tearing (Milgrom et al. 1992). Full-thickness tears usually occur in diseased tendons. Areas of friction, impingement, and force concentration during contraction are important in the development of chronic mechanical damage and tendinopathy. Some authors believe that areas of relatively poor vascular supply (e.g., the mid-Achilles tendon) also are predisposed to tendinopathy owing to impaired tendon healing (Milgrom et al. 1992).
Anterior impingement of the ankle may occur secondary to either an osseous or soft tissue lesion. Osseous impingement is due to osteophyte formation in the talus or anterior tibia. As well as being common in kicking sports, this condition is also seen in ballet dancers as it occurs in activities that involve forced dorsiflexion of the ankle joint. Soft tissue impingement is due to fibrous connective tissue formation and impingement in the anterolateral or anteromedial ankle following a sprain (Gall et al. 2008; Speed 1998; Alonso et al. 2010).
41.5.11 Foot Injuries
These fractures are a result of chronic stress due to vertical loads on the proximal third of the metatarsal shaft. Stress fracture of the fifth metatarsal, in particular, is not an uncommon injury in basketball players. Metatarsal stress fractures can occur in any sport that has repetitive jumping, landing, and cutting maneuvers, but basketball players has highest incidence of metatarsal injuries (Speed 1998; Alonso et al. 2010; McBryde 1985; Brukner et al. 1996).
Midfoot sprains usually are caused by a sudden rotation of a planted foot or an axial load on a plantar flexed foot. The classic mechanism involves a football player whose foot is planted with the toes extended and ankle plantar flexed.
Base of the fifth metatarsal fractures is subjected to fracture. This could be due to direct trauma, avulsion fracture, or diaphyseal stress fractures (Knobloch et al. 2007). Most of these fractures are non-displaced; they may be managed symptomatically.
Plantar fasciopathy is degenerative tendinopathy of the plantar fascia, which runs from the heel to the middle of the foot. This condition is common in long-distance runners and walkers (Milgrom et al. 1992).
41.5.12 Stress Fractures
Fatigue stress fracture was first described in military recruits (Jones et al. 2002; Speed 1998; Matheson et al. 1987; Gilbert and Johnson 1966). Stress fractures are overuse injuries often seen in athletes who perform high-repetition, low-impact activities, such as running, jumping, and swimming (Fahlström and Söderman 2007; Knobloch et al. 2007; Clanton and Solcher 1994; Pell et al. 2004; Chang and Harris 1996). The fractures occur when the normal bone is subjected to a frequent repetition of repetitive subthreshold forces, and the natural reparative mechanism is overloaded (Jones et al. 2002; Speed 1998; Knobloch et al. 2007; Giladi et al. 1987). Those particularly affected are military recruits and athletes (e.g., runners, dancers, and basketball players) (Jones et al. 2002; Speed 1998). Fractures usually occur during or up to 4 weeks after the commencement of preseason training (Knobloch et al. 2007; Giladi et al. 1985).
41.5.12.1 Pathophysiology of Fatigue Stress Fractures
When the bone is subjected to stress, it attempts to become stronger by remodeling its internal architecture (Jones et al. 2002; Speed 1998). Initially there will be an early osteoclastic resorption of the bone at the area of mechanical stress causing weakening of the bone (Matheson et al. 1987; Belkin 1980; Dugan and D’Ambrosia 1983). This will be followed by another phase in which osteoblastic activity increases to balance the resorption and improve strength along the stress line (Jones et al. 2002). However, during the lag time between these two phases, the bone is also more susceptible to fracture. If excessive stress continues during this remodeling, then “stress reactions” occur, involving plastic deformation of the bone (Jones et al. 2002; Matheson et al. 1987; Belkin 1980; Dugan and D’Ambrosia 1983; McBryde 1985).
41.5.12.2 Incidence of Stress Fracture in Female Athletics
Reporting of stress fractures among female athletes is increasing, predominately because of the ever-increasing mass participation in sporting and increasing the number of female recruitment in the military (Jones et al. 2002; Speed 1998; Arendt et al. 2003; Knobloch et al. 2007; Hoch et al. 2005; Bennell and Brukner 1997).
Studies of military recruits report an incidence varying from 2 to 64 % in different countries (Speed 1998; Slauterbeck et al. 2002). In one report, estimates of stress fracture rates of 5–12 % have been reported among women undergoing various entry-level military training programs, rates that are about 1.5–5 times higher than those reported for men undergoing similar training (Arendt et al. 2003; Bennell and Brukner 1997; Jones et al. 1993). More important, pelvic and femoral stress fractures, more common among women than among men in military settings, have a higher frequency of complications (Campbell and Warnekros 1983; McKenzie et al. 1985; Frnsztajer et al. 1990). Stress fractures may comprise as much as 10–15 % of all sports injuries (Arendt et al. 2003; Bennell et al. 1996) and between 4.7 and 20 % of injuries to runners (Arendt et al. 2003; Bennell et al. 1996; James et al. 1978).
41.5.12.3 Risk Factors for Stress Fracture
Risk factors for stress fracture do not differ from those for other overuse injuries. Biomechanics and alignment are important factors in the etiology of stress fracture (Matheson et al. 1987; James et al. 1978). The rigid pes cavus foot was found to be more common in stress fractures of the metatarsal and femur (Matheson et al. 1987). Tarsal bone stress fractures were also common in individuals with pronated feet (Matheson et al. 1987; Campbell and Warnekros 1983; McKenzie et al. 1985). Low aerobic fitness was strongly associated with consequent stress fracture injury (Beck et al. 2000).
Military recruits have higher rate and different patterns of stress fractures from those found in athletes (Matheson et al. 1987). Military recruits often have a lower degree of musculoskeletal fitness at the time of injury and are required to march in hard footwear, train on cement or asphalt surfaces, and have a markedly emphasized heel strike (Matheson et al. 1987). The rate of loading of the musculoskeletal system in military recruits is rapid, and the pattern of loading associated with marching is distinct. It is likely that military recruits have specific patterns of injury, which reflect these factors (Matheson et al. 1987).
41.5.12.4 Site of Athletic Stress Injuries
Stress fracture can almost affect any bone in the body (Jones et al. 2002). Stress fractures of the lower extremity account for 80–95 % of all stress fractures (Jones et al. 2002; Knobloch et al. 2007; Boden et al. 2001; Sterling et al. 1992). Running, however, appears to be the most commonly reported sport or exercise activity associated with the occurrence of stress fracture (Jones et al. 2002). Stress fractures account for 4–16 % of running injuries (Jones et al. 2002; Speed 1998). Stress fractures may be associated with a specific sport such as the humerus in throwing sports, the ribs in golfers and rowers, the spine in gymnastics, the lower extremity in running activities, and the foot in gymnastics and basketball. Stress fractures in athletes differ clinically from stress fractures in the military population (Verma and Sherman 2001; Brukner et al. 1996). The radiographic and pathologic findings do not differ. The most striking clinical differences are in the incidence and site (Angus and McBryd 1976).
The majority of stress fractures involve the tibia (Jones et al. 2002; Knobloch et al. 2007) (Fig. 41.1) (around 50 %) mainly in the proximal metaphyseal (Fig. 41.2) or upper diaphyseal (Fig. 41.3) (Wojtys et al. 1998; Touliopolous and Hershman 1999; Boden et al. 2001; Sterling et al. 1992) followed by the metatarsal bones (occurring in about 10–20 % of athletes, particularly runners) and then the fibula and the tarsal navicular bone (Fig. 41.4) (Speed 1998; Knobloch et al. 2007).
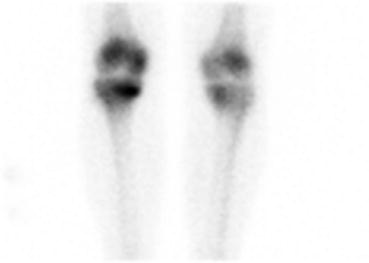
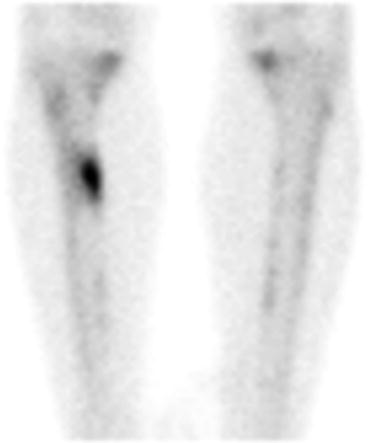
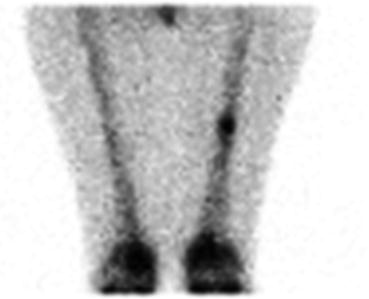
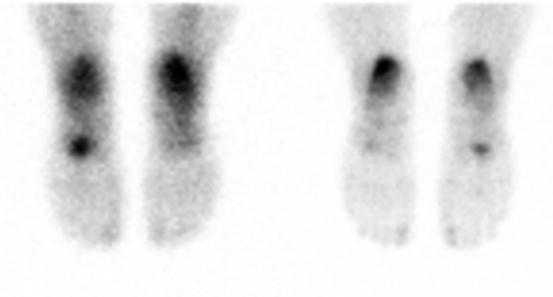
Fig. 41.1
Medial plateau stress fracture in a female military recruit
Fig. 41.2
Metaphyseal stress fracture in a female military recruit
Fig. 41.3
Diaphyseal stress fracture in a female military recruit
Fig. 41.4
Navicular stress fracture in a female military recruit
Stress fractures are far less common in the upper extremity than in the lower extremity, but fractures have been described in athletes participating in throwing sports, tennis, and swimming (Wojtys et al. 1998; Adolfsson and Lysholm 1990; Farquharson-Roberts and Fulford 1980; Murakami 1988).
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


