The testes are located in the scrotum in 90% of full-term infants. When not in the scrotum, they are usually to be found within the inguinal canal. Rarely, they are intra-abdominal. Testicular size varies with age and with the onset of puberty. US is the gold standard for evaluating the testis and epididymis as it can demonstrate changes in size and texture, as well as assessing blood flow using spectral and color Doppler. NM (99m Tc pertechne-tate) has been used in cases of suspected torsion, but as it uses radiation it is not usually recommended. MRI can also assess the testis but is rarely indicated because of the cost.
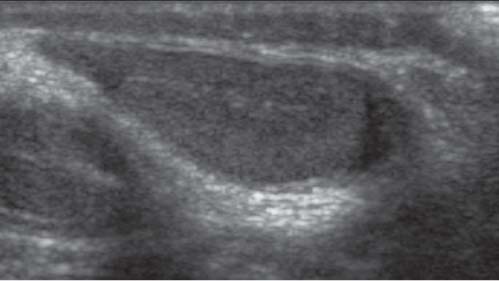
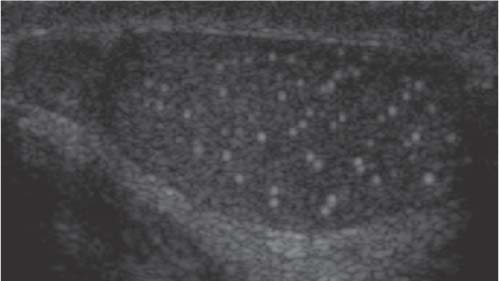
On US, the normal testis is primarily of homogeneous echo-genicity (Fig. 3.59). A not uncommon finding is microcalcification within the testicular parenchyma (Fig. 3.60) and is usually of no clinical significance.
An undescended testis, seen in 0.5% of boys prior to puberty, is the most common abnormality seen. Congenital aplasia of one testis is rare, and bilateral aplasia is very rare. US is the modality of choice to search for the testes, but if they are not within the inguinal canal they may be diff cult to see within the abdomen due to bowel gas; in that case, MRI may be useful.
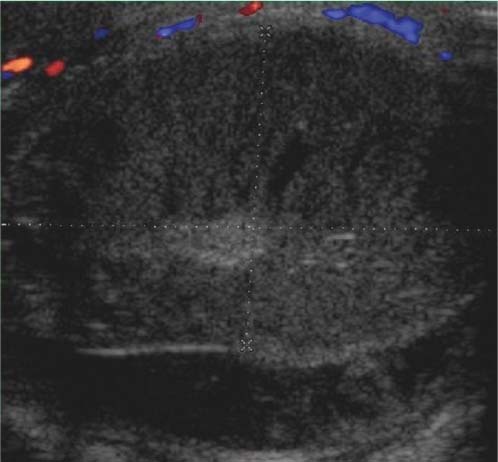
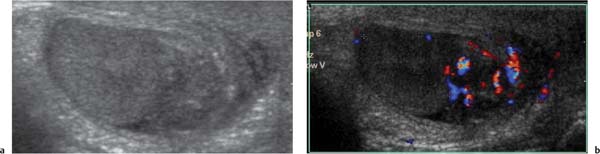
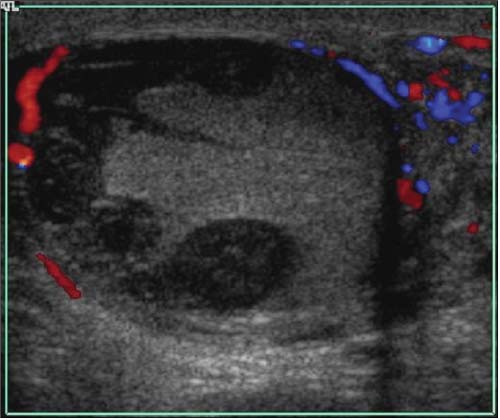
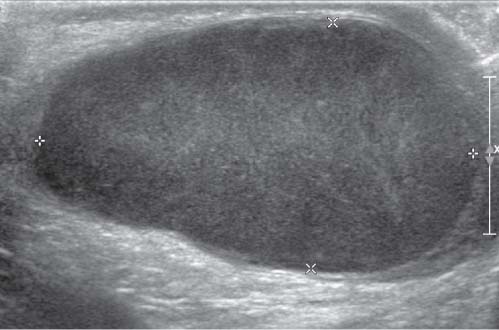
If there is scrotal swelling without pain or inflammation, the most common cause is a hydrocele (Fig. 3.61). If there is pain and/or evidence of inflammation, then testicular torsion has to be the first consideration, as this is a surgical e mergency. Testicular torsion is indicated if there is disorganization of the echo texture, usually enlarged and hypoechoic, (Fig. 3.62) with loss of blood flow within the testis on color Doppler; however, this is not always reliable, particularly if the torsion is intermittent. The most common radiologic diagnosis with an acutely tender testis is epididymitis (with or without orchitis). Seeing marked increase in blood flow to a swollen epididymis on color Doppler can make the diagnosis (Fig. 3.63). If the testis is involved with increased blood flow, then it is orchitis as well as epididymitis. Torsion of the testicular appendage is the other diagnosis to be considered and is seen as a swollen appendage separate from the epididymis. Torsion is the most common cause in infants and adolescents, and 50% of boys with torsion of the testicular appendage are between 9 and 12 years old.
Trauma can result in testicular hematomas. These can remain for an extended period of time and hence be mistaken for a more sinister lesion (Fig. 3.64). If there is a patent processus vaginalis, herniation of bowel loops or fluid from the perito-neal cavity can occur and extend into the scrotum. This can also happen with meconium peritonitis resulting in calcification.
Tumors are rare before puberty. The most common involvement of the testis by tumor is in leukemia.
Fig. 3.59 Normal testis. Normal echotexture shown on US.Fig. 3.60 Testicular microlithiasis. Microcalcification is seen sono- graphically as multiple echogenic foci.Fig. 3.61 Hydrocele. The fluid extent is well shown by US in a young infant boy.Fig. 3.62 Testicular torsion with infarction. The testis is enlarged and hypoechoic, with no flow on color Doppler study.Fig. 3.63a, b Right epididymitis. The epididymis is enlarged and of mixed echogenicity (a) and shows marked increase in blood flow on color Doppler study (b).Fig 3.64 Testicular trauma. Multiple hypoechoic areas are seen in the testis, which has a mixed echotexture.
Table 3.23 Testicular enlargement
Diagnosis
Findings
Causes and comments
Hypertrophy
Homogeneously enlarged testes of normal echogenicity on US.
Atrophy or agenesis of the contralateral testis; bilateral hypertrophy is caused by hormone-secreting tumors.
Enlarged hypoechoic testes with decreased or absent perfusion on color Doppler and scintigraphy. Not 100% reliable as torsion can be intermittent with flow returning intermittently.
Torsion of the vascular pedicle with resultant necrosis of the testis. Peak incidence in the neonatal period and in adolescence.
Testicular appendage torsion
Testis and epididymis are normal with a swollen appendage showing increased vascularity on color Doppler.
Torsion of the vascular pedicle and resultant necrosis of the appendage.
Enlarged epididymis, compared with the opposite side, fluid in the scrotal sac on US. Often shows markedly increased perfusion on scintigraphy and color Doppler.
Orchitis, postcatheterization, cystoscopy. Rarely due to ectopic insertion of the ureter into ductus deferens.
Orchitis
Testis and epididymis are enlarged with irregular echogenic parenchyma and increased vascularity on color Doppler.
Various histology, such as teratoma, embryonal cell carcinoma, seminoma, gonadoblastoma, rhabdomyosarcoma.
Adrenogenital syndrome
Focally decreased parenchymal echogenicity and calcification on US. The epididymis is enlarged and lobulated; micro-adenomas develop later.
Caused by insufficient replacement therapy.
Fig. 3.65 Testicular teratoma. Enlarged testis without focal lesions. There is markedly inhomogeneous and disorganized echotexture of the parenchyma.Fig. 3.66 Testicular teratoma.
Table 3.24 Small testes
Diagnosis
Findings
Comments
Atrophy
Diminished volume of one or both testes, echogenicity normal or decreased on US; hypertrophy of the contralateral testis.
Can occur after torsion, incomplete descent, orchitis, or orchidopexy. Also seen in cystic fibrosis and Kartagener syndrome.
Hypoplasia
Testes are small on US.
Associated with prune belly syndrome, cystic fibrosis, and chromosomal abnormalities or as late sequelae of radiation or chemotherapy.
Only gold members can continue reading. Log In or Register to continue