Abstract
Ventricular septal defects (VSD) are the most common cardiac defects (25%–30% of newborns), being frequently associated with more complex congenital heart defects (10% of fetuses with cardiac defects). The diagnosis of fetal VSD can be difficult, in particular for small and isolated VSDs, which must be actively sought on routine morphologic scans. Color and pulsed wave Doppler may be very helpful to establish the location and size of the VSD. Although the clinical prognosis of isolated VSD is usually good, an extensive workup is required to rule out chromosomal abnormalities, other structural abnormalities, and genetic syndromes present in 25%–35% of the cases. Inlet, perimembranous, malalignment, and large VSDs (>50% of the aortic lumen) are particularly associated with chromosomal abnormalities, whereas the risk is not increased for isolated muscular VSDs, especially in gestations with a normal first-trimester screening test for aneuploidies. Overall prognosis is good for isolated VSD. The obstetric management should not be changed; patients can deliver in their local hospital.
Keywords
ventricular septal defect, perimembranous defect, muscular defect, echocardiography, Doppler
Introduction
Ventricular septal defect (VSD) is the most common congenital heart disease (CHD) in children and adults. VSD is present in 25% to 30% of newborns with a CHD. VSD can frequently occur in combination with other CHDs, as part of complex heart defects, which are discussed in Chapters 76 , 77 , 83 , and Chapter 85 , Chapter 86 , Chapter 87 , Chapter 88 . This chapter addresses the prenatal features of isolated VSDs.
Disease
Definition
VSDs are openings in the ventricular septum that freely communicate between the left and right ventricles. These defects are classified according to their location in the ventricular septum and may involve one or more components of the septum. The particular location of the defect has no bearing on the direction of the intracardiac shunt but has significant predictive value in terms of the frequency of involvement of the semilunar or atrioventricular valves, associated anomalies, and spontaneous closure.
Prevalence and Epidemiology
The incidence of VSD ranges from 3 : 1000 to 5 : 1000 live births. VSD is the most common form of CHD in childhood. Although VSDs represent approximately 25% to 30% of all CHDs at birth, they are often unrecognized in utero, accounting for only 5% to 7% of all prenatally diagnosed CHDs.
Etiology and Pathophysiology
The etiology is multifactorial. Although only a few VSDs are associated with chromosomal abnormalities in the child, when a VSD is diagnosed in the fetus, the risk of chromosomal abnormalities is much greater (5% to 10%, especially in large or perimembranous VSD). VSD can frequently occur in combination with, and may lead to the diagnosis of, other CHDs and extracardiac malformations. The prenatal diagnosis of VSDs may be of great clinical relevance.
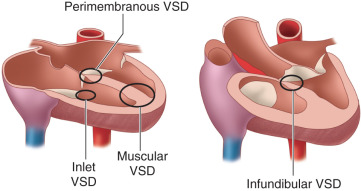
There are four types of VSD ( Fig. 75.1 ):
- 1.
Perimembranous VSD (70%–80%, also called paramembranous or infracristal ): located in the membranous septum, which is the base of the heart between the inlet and the outlet components of the muscular septum.
- 2.
Inlet VSD (<5%, also called posterior or lower ): involving the inlet muscular septum, which is inferior-posterior to the membranous septum.
- 3.
Muscular VSD (15%–20%): located in the trabecular muscular septum; can also be classified as midmuscular (superior to the moderator band) and apical (inferior to the moderator band).
- 4.
Infundibular VSD (<5%, also called outlet, supracristal, choanal, conoventricular, subpulmonary, or doubly committed subarterial defects ): located in the infundibular muscular septum, which is the portion of the septum separating the right and left ventricular outflow tracts.
Manifestations of Disease
Clinical Presentation
The presence of an isolated VSD in utero has little effect on the normal cardiac physiology because pressures generated in each ventricle are quite similar, leading to minimal shunting of blood despite even large ventricular communications. When the infant is delivered, there is an immediate decrease in pulmonary vascular resistance and lower pressures in the right ventricle, whereas the left ventricle contracts against high systemic vascular resistance, generating higher pressures. A left-to-right shunt results, the magnitude of which is influenced by the size of the defect, the pressure in the right and left ventricles, and the pulmonary resistance. Over time, large defects may lead to Eisenmenger syndrome with pulmonary hypertension, in which elevated pulmonary artery pressure eventually leads to reversal in the direction of shunting, desaturation, cyanosis, and secondary erythrocytosis.
Imaging Technique and Findings
Ultrasound.
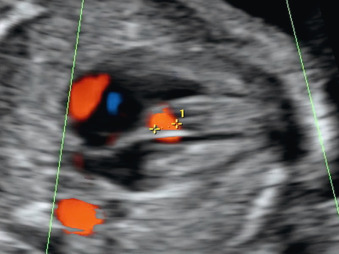
A VSD appears on ultrasound (US) as an interruption of the septum. If the VSD is small, it can be very difficult to identify. It is often hard to define the size and course of the VSD because the muscular septum is a three-dimensional structure, and the defects may be tortuous and multiple.
The best echocardiographic view for diagnosis depends on the site of the VSD. The four-chamber view can identify perimembranous ( Fig. 75.2 ), inlet, and muscular VSDs ( Fig. 75.3 ), and the five-chamber left ventricular outflow tract view can detect infundibular VSDs ( Fig. 75.4 ). Infundibular VSDs can be divided into two types according to whether the remaining septum caudal to the defect and the aortic wall are aligned (simple infundibular defect) or not (malalignment VSD) ( Fig. 75.5 ).