24 Anatomy and Craniocervical Junction
24.1 Spine Anatomy
The vertebral column is the central supportive structure of the body, linking the skull base to the pelvis, with the ribs and extremities connected directly to the periphery of the column or connected indirectly to it through other bones, such as the shoulder or pelvic girdle. The vertebral column also serves to protect the spinal cord, and is a defining anatomic feature of higher-order life forms. In addition to the structure and protection provided by the bones of the vertebral column, the fibrocartilagenous intervertebral disks provide the ability for movement.
The vertebral column consists of 24 articulating vertebrae, including 7 cervical (C1–C7), 12 thoracic (T1–T12), and 5 lumbar vertebrae (L1–L5), and 9 fused and relatively immobile vertebrae, including 5 sacral (S1–S5) and 4 coccygeal (Cx1–Cx4) segments. The morphology of the coccyx is highly variable, and there are often transitional vertebrae at the lumbosacral junction, typically a sacralized (or hemisacralized) L5 vertebra or a lumbarized (or partly lumbarized) S1 vertebra. There are also variations in the number of ribs, including occasional cervical ribs at C7, absent ribs at T12, or rudimentary ribs at L1. Throughout the articulating portions of the vertebral column, the vertebrae are separated from one another by fibrocartilagenous intervertebral disks. At each vertebral level are right and left nerve roots that emanate from the neural foramen. In the cervical spine, the C2–C3 neural foramen carries the C3 nerve root, and in the thoracic spine (as in the lumbar and sacral regions) the T1–T2 neural foramen carries the T1 nerve root. At the cervicothoracic junction is a C8 nerve root, although there is no C8 vertebra. Also, although the coccyx has four osseous segments, there is only one coccygeal nerve.
24.1.1 Typical Articulating Vertebrae
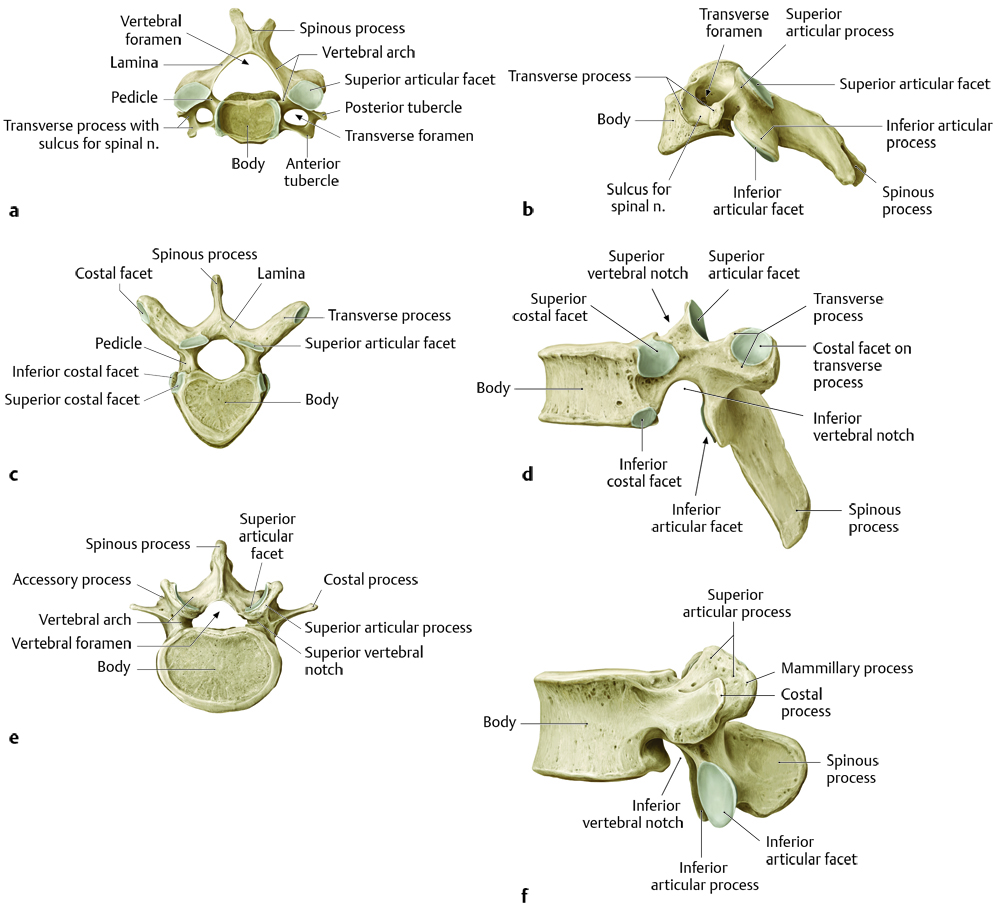
The articulating vertebrae have a vertebral body and a posterior neural arch. The posterior neural arch consists of two pedicles that extend posteriorly to the superior and inferior articulating facets. Posterior to that are medially directed laminae that come together to form the posteriorly directed spinous processes. Beneath the pedicles of the neural arch are the neural foramina, through which nerve-root sleeves project. (It is a satisfaction in pediatric neuroradiology to almost never have to describe neural foraminal stenosis, except at the apex of a severe scoliotic curvature and in several other rare situations.) The vertebrae have laterally directed transverse processes that arise anterior to the facets in the cervical and lumbar spine and posterior to the facets in the thoracic spine (Fig. 24.1).

24.1.2 Special Anatomic Considerations
The first two cervical vertebrae have unique morphologic and functional characteristics. The first cervical vertebra, C1, does not contain a vertebral body, and represents a ring. The ring has an anterior and posterior neural arch, with two lateral masses. These lateral masses articulate with the occipital condyles, and because the C1 vertebra supports the cranium, it is sometimes referred to as the atlas (derived from the name of Atlas, the Greek god who supported the world on his back). The articulation of the atlas with the occipital condyles allows vertical motion of the head (e.g., nodding of the head) (Fig. 24.1a,b; Fig. 24.2, Fig. 24.3, Fig. 24.4, Fig. 24.5).




The body of the C2 vertebra has a superiorly directed vertical protrusion known as the odontoid process (also known as the dens). The odontoid process serves as a post around which C1 can rotate, and by allowing such rotation of the head, C2 is also known as the axis. The posterior neural arch of C2 is similar to those of C3–C7, described above.
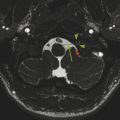
The vertebral bodies of C2 through C7 do not have a purely planar inferior surface, because the side edges of the vertebrae immediately below each of these vertebrae have the hook-shaped processes known as uncinate processes, which prevent C2 through C7 from sliding backward and off the surfaces of C3 through T1, respectively. This provides an additional articulation known as the uncovertebral joint. Each of the cervical vertebrae also has within its transverse processes an opening known as the foramen transversarium through which the left and right vertebral arteries pass (typically entering at approximately the C6 level) before merging within the skull to form the basilar artery. In summary:
The thoracic vertebrae articulate with ribs.
The lumbar vertebrae typically do not have any special features.
The sacral vertebrae are typically fused with one another without a formed disk space between them. Instead of transverse processes, the sacral vertebrae have winglike lateral projections (alae).
The coccyx is largely ignored when evaluating imaging of the spine.
24.1.3 Alignment
The adult cervical spine typically has a mild lordosis, with a mild kyphosis in the thoracic spine and a mild lordosis in the lumbar spine. In childhood, the cervical alignment is often straight or slightly kyphotic, which is normal (see Chapter 28 for further discussion). It is important to also be aware of an additional variant in spinal alignment in young children, which is the apparent subtle (up to approximately 3 mm) anterolisthesis of C2 with respect to C3, known as pseudosubluxation (Fig. 24.6). It is normal for children under approximately 8 years of age to have a subtle alignment variant at this location, and this should not be mistaken for a fracture.

24.1.4 Ligaments
The anterior surfaces of the vertebrae are connected by a continuous anterior longitudinal ligament (ALL). The posterior margins of the vertebral bodies, which together form the anterior margin of the spinal canal, are connected by the posterior longitudinal ligament (PLL). The posterior/posterolateral margin of the spinal canal consists of the ligamenta flava, which connect the laminae of adjacent vertebrae. Between the spinous processes are interspinous ligaments, and overlying the tips of the spinous processes, from C7 to the sacrum, is the supraspinous ligament.
The ALL extends to the anterior surface of the clivus, at the skull base, as the anterior atlanto-occipital ligament. The PLL extends superiorly from the odontoid process as the tectorial membrane, where it becomes the dorsal dura of the clivus, and the ligamentum flavum extends superiorly to the posterior margin of the foramen magnum (opisthion) as the posterior atlanto-occipital ligament. The supraspinous ligament in the upper cervical spine does not remain adjacent to the tips of the spinous processes, and is known as the nuchal ligament, attaching to the occipital bone at the external occipital protuberance.
The tip of the odontoid process has a ligamentous connection, known as the apical ligament of the odontoid, that extends superiorly to the basion. Two superior-oblique ligaments, the alar ligaments, extend from the odontoid process to the occipital condyles. A horizontally oriented ligament connecting both sides of the anterior neural arch of C1 and extending posterior to the odontoid process is the transverse ligament.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


