4.3 Unusual Fractures
4.3.1 Case 61 (Fig. 4.19)

Case description
Referral: self-referred by the patient.
Prior history and clinical question: The patient claimed an approximately 6-week history of low back pain radiating to the right leg. Until several years previously, he participated in competitive sports.
Radiologic Findings
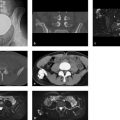
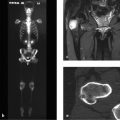
Imaging shows a small osteolytic lesion with sclerotic margins in the right posterior ilium. A lucent track, which resembles a gaping fracture line, extends medially downward from the osteolytic focus to the adjacent sacroiliac joint. The joint appears normal, especially on its sacral side, in all CT sections (Fig. 4.19 a, d–f) and on MRI (Fig. 4.19 b, c). Caudal to the bony lesion is a circumscribed area of edema-like signal within the bone (Fig. 4.19 b, c). MR images of the lumbar spine (not pictured here) clearly demonstrated a mediolateral disk herniation at the L5–S1 level on the right side.
Location
The changes described above are located entirely within the cancellous bone and occupy an area of the posterior pelvic ring that is subject to large physiologic loads (anterior superior corner of the ilium).
Pathoanatomic Background of the Findings
It is clear that, particularly in Fig. 4.19 f, a small triangular bone fragment has separated from the surrounding bone. Lateral to the fragment is a bone defect that may be interpreted as an area of resorption or destruction.
Assignment to a Possible Basic Entity
Normal variant?
No known precedent.
Trauma?
Very likely. The patient was a competitive athlete, and it would not be unusual for a stress fracture to develop in the anterior superior corner of the posterior ilium leading to necrosis and separation of a small triangular bone fragment. Accordingly, the small osteolytic focus in the coronal reformatted CT image (Fig. 4.19 a) would represent a resorption zone lateral to the fragment seen in the magnified axial view (Fig. 4.19 f). The marginal sclerosis suggests an older process, which would be consistent with the patient’s history. The edema-like signal, lateral and caudal to the main focus, could reflect a certain instability of the bone fragment. It should not be interpreted as the cause of the pain. Many ill-defined hyperintensities in water-sensitive sequences (edema-like signal, not bone marrow edema, see Ill-Defined Hyperintensity in Chapter ) are known to have no clinical relevance.
Inflammation?
No, the location at a peripheral site in the ilium of an adult would be extremely unusual.
Tumor?
No, it is difficult to conceive of a tumor (eosinophilic granuloma, non-Hodgkin lymphoma?) that would cause necrosis and separation of a bone fragment.
Necrosis?
To a degree; see under Trauma? above. To the author’s knowledge, the occurrence of primary necrosis has not previously been described in this region, which is not a terminal vascular bed. The patient is not known to have any diseases or other factors (e.g., corticosteroid use) that would predispose to osteonecrosis.
Synopsis and Discussion
The osteolytic lesion is probably an incidental finding, as the 6-week pain history is more consistent with a radicular process relating to a herniated nucleus pulposus at L5–S1. When specifically questioned, the patient claimed that his symptoms resolved within days after taking a nonsteroidal anti-inflammatory drug. This also points to a radicular cause.
In summary, the history of competitive sports participation suggests a previous stress fracture that did not heal completely and caused necrosis leading to the separation of a small bone fragment. Because the marginal sclerosis appears to be of long standing (see section on Trauma? above), it is reasonable to assume an earlier onset of clinical manifestations, perhaps several years ago.
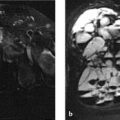
Follow-up MRI at 2 years documented complete consolidation of the stress fracture (Fig. 4.20).

Working Diagnosis
Old, unhealed stress fracture in the anterior superior corner of the ilium.
Comments
The clinical relevance of an imaging abnormality can be determined only by considering the patient’s history. In this case the patient had two radiologic findings (herniated disk plus a bony lesion of the ilium) with only one dominant clinical complaint: low back pain with radicular symptoms. The radiologist must now consider what diagnosis is congruent with these findings, aided by consultation with the referring clinician whenever possible.
4.3.2 Case 62 (Fig. 4.21)


Case description
Referring physicians: trauma surgeon and internist (endocrinologist).
Prior history and clinical question: A 66-year-old woman presented with diffuse skeletal and muscle pain that rendered her unable to walk. She lived alone. An internist diagnosed hepatopathy of unknown cause. She reportedly suffered recurrent bone fractures following trivial trauma. We ordered laboratory tests which showed a greatly elevated alkaline phosphatase level.
Radiologic Findings
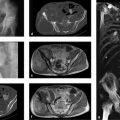
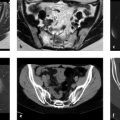
The plain radiographs (Fig. 4.21 a, b) show a “butterfly” pattern of fractures in the anterior pelvic ring with progressive displacement from May to December of 2009 and associated callus formation that is exuberant for the age of the patient. The bones of the posterior pelvic ring show structural alterations that CT (abdominal examination in May, 2009) identifies as large fracture gaps with surrounding reactive-reparative sclerosis in the sacrum (Fig. 4.21 d–f, h–k). The images in Fig. 4.21 g–i demonstrate a fracture of the right pubic ramus; highly structured ossifications are projected anterior and lateral to the fracture site (see also Fig. 4.21 l). A radiograph of the right foot taken in May of 2009 (Fig. 4.21 c) shows a broad, incomplete fracture at the base of the fifth metatarsal. Axial CT scans of the bony thorax (Fig. 4.21 m, n) show rib fractures that are unhealed despite callus formation. CT scans of the spine (not pictured here) did not show spinal fractures.
Location
The principal fractures are located in the anterior and posterior pelvic ring and at the anterior and posterior bends of the rib cage.
Pathoanatomic Background of the Findings
Unhealed fractures in skeletal regions exposed to large mechanical loads (anterior and posterior pelvic ring, bends of the rib cage, base of the fifth metatarsal) in patients without a significant trauma history are always suspicious for insufficiency fractures, or fractures occurring in structurally weakened bone as in osteomalacia. The ossifications about the right pubic fracture may be heterotopic ossifications due to hemorrhage.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


