4.4 Bone Lesions with a Predominantly Extraosseous Component
4.4.1 Case 65 (Fig. 4.27)

Case description
Referring physician: orthopedist.
Prior history and clinical question: A 29-year-old man presented with rapidly increasing pain and swelling in the right gluteal region.
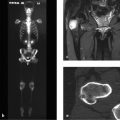
Radiologic Findings
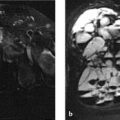
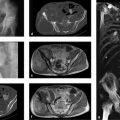
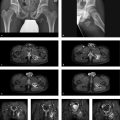
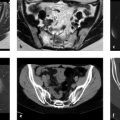
CT demonstrates a broad-based ossified lesion on the right ilium that communicates directly with the medullary cavity with no intervening cortex (Fig. 4.27 b). The attenuation values inside the lesion are like those in the adjacent medullary cavity (Fig. 4.27 b, f). The lesion is surrounded peripherally by a grotesque soft-tissue mass that is inhomogeneously dense on CT and less dense on average than the muscles (Fig. 4.27 c–f). Scattered calcifications are visible within the mass (arrows in Fig. 4.27 d). MRI (Fig. 4.27 a, T2w fat-suppressed image) shows a fine linear hyperintensity that directly abuts the ossified mass. The large mass is hypointense to muscle and is encircled by an irregular, hyperintense rim of nonuniform thickness.
Location
The ossified lesion on the ilium is in direct contact with the medullary cavity of the underlying bone, that is, the medullary cavities of the exostotic lesion and the ilium communicate with each other.
Pathoanatomic Background of the Findings
It is not difficult to describe the lesion on the ilium as an exostosis. Because the medullary cavities of the “parent” bone and exostosis communicate with each other and the exostosis is bordered by a thin film of hyperintense material that is isointense to cartilage, we are dealing with a cartilaginous exostosis (osteochondroma). By its volume alone, the surrounding grotesque soft-tissue mass appears to be sarcomatous tissue that is rimmed by hyperintense tumor cartilage. But is this necessarily true?
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


