5.1 Clavicle
5.1.1 Case 78 (Fig. 5.1)

Case description
Referring physician: orthopedist.
Prior history and clinical question: A 21-year-old man was examined radiologically for multiple injuries. A radiograph of the left clavicle showed a defect in the inferior border just lateral to the head of the clavicle (the medial or sternal end of the clavicle). Before ordering biopsy, the orthopedist wanted to know what the defect might represent.
Radiologic Findings
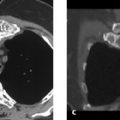
A semicircular defect is visible in the inferior border of the clavicle just lateral to the clavicular head (see arrows in Fig. 5.1 a). A subsequent whole-body bone scan (Fig. 5.1 b) appears normal. Slightly increased uptake in the manubriosternal synchondrosis is considered appropriate for age.
Location
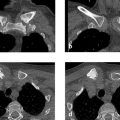
The defect is located at the attachment of the costoclavicular ligament. This was also seen in CT scans, which are not reproduced here because the case can be solved without them (see Assignment to a Possible Basic Entity below). A similar but very subtle finding was also noted on the contralateral side.
Pathoanatomic Background of the Findings
The tissue structure replacing the bone is not associated with increased bone turnover (negative bone scan)—that is, it does not incite a perifocal reaction, and it does not form a matrix (e.g., bone, cartilage, ossifying connective tissue).
Assignment to a Possible Basic Entity
Normal variant or malformation?
Yes. The very fact that the defect was detected incidentally and was negative on the bone scan suggests a normal variant. When we consider its location (see above), it is reasonable to assume that we are dealing with a normal variant.
Trauma, inflammation, tumor?
The negative history and negative bone scan exclude these basic entities from a realistic differential diagnosis.
Synopsis and Discussion
The apparent defect in the undersurface of the clavicle, just lateral to the medial end of the clavicule (clavicular head), is called a “ligament groove” in the literature and corresponds to the attachment of the costoclavicular ligament.17 This attachment site generally appears radiographically as a more or less pronounced irregularity in the contour of the bone. In extreme cases it forms an actual groove and appears as a well-defined defect, especially when the shoulder girdle has been subjected to particularly high mechanical stresses. This is not necessarily an insertional tendinopathy in the form of a rarefying fibro-ostosis, as this would show at least slightly increased tracer uptake on the bone scan. Similar findings are known to occur in the femoral neck (see Case 69 and Case 73), the ischia, at the pectoralis attachment (see images in Case 102, Case 103, and Case 104), and at other sites.
Final Diagnosis
Ligament groove at the attachment of the costoclavicular ligament, considered a normal variant.
Comments
The key to the correct interpretation of a radiologic finding often lies in its location.
5.1.2 Case 79 (Fig. 5.2)

Case description
Referring physician: radiologist.
Prior history and clinical question: A 37-year-old woman, otherwise healthy, felt a lump in her left supraclavicular fossa. She stated that many years ago she had suffered head and neck sprains in a motor vehicle accident but could recall no further details. The radiologist wanted to know the origin of the finger-shaped structure at the junction of the neck and shoulder. Malformation?
Radiologic Findings
The radiograph in Fig. 5.2 shows a finger-shaped bony structure that follows the lateral border of the trapezius muscle and widens from above downward in a trapezoidal pattern. A kind of pseudarthrosis is noted at the center of the structure. The acromial end of the clavicle shows pencil-like tapering and is surrounded by a club- or cuff-shaped ossification.
Location
As stated above, the ossified structure follows the lateral border of the trapezius muscle. The peripheral end of the left clavicle has vanished. In terms of vascular anatomy, this area represents a terminal vascular bed with a critical blood supply. The finger-shaped ossification on the lateral side of trapezius appears connected to the lateral cuff-shaped structure by the clavicular attachment of the trapezius muscle.
Pathoanatomic Background of the Findings
The oblong structure at the lateral junction of the neck and shoulder is composed of solid bone with a cortex and medullary cavity, causing it to resemble a finger. The bony cuff around the tapered peripheral clavicle is also composed of solid bone.
Assignment to a Possible Basic Entity
Normal variant or malformation?
A kind of accessory bone called the os omovertebrale (Latin om = shoulder) located at the junction of the shoulder and lateral neck has been described in the literature.17 It is known to occur in Klippel–Feil syndrome. The finger-shaped bony structure could very well be an os omovertebrale, but the cervical vertebrae that appear in the radiograph do not show any gross signs of Klippel–Feil syndrome such as blocking. Could this be due to trauma?
The ossifications could be a result of old myositis ossificans (heterotopic ossification) caused by trauma. This would be consistent with the patient’s history.
Inflammation or tumor?
This diagnosis would not be consistent with the clinical presentation or radiologic findings.
Synopsis and Discussion
The finger-shaped structure most likely represents a mature form of myositis ossificans traumatica. The pseudarthrosis is explained by its location, which is the site that undergoes the greatest deformation when the arm is raised and lowered. A diagnosis of myositis ossificans traumatica is also supported by the changes in the peripheral clavicle: The trauma probably caused a fracture of the peripheral clavicle or an acromioclavicular joint separation, leading to the development of avascular acro-osteolysis or acronecrosis (see also Case 93), which is a fairly common result of trauma to the peripheral clavicle. The “licked candy stick” appearance is considered proof of acro-osteolysis or acronecrosis. The club-shaped ossification around the tapered peripheral end of the clavicle probably also represents a mature myositis ossificans.
Fig. 5.3 a–c illustrates another case of heterotopic ossification (myositis ossificans traumatica) in the shoulder girdle. The 62-year-old patient suffered a serious shoulder injury with rupture of the left acromioclavicular joint, as documented on the posttraumatic radiograph in Fig. 5.3 c. With a 10-kg weight held in each hand, the distance between the superior border of the coracoid process and the inferior border of the clavicle is two times greater on the left side than on the right—a sure sign of a Tossy stage III acromioclavicular joint rupture. At follow-up 1 year later, a radiograph of the left acromioclavicular joint (Fig. 5.3 b) showed bone formation between the left clavicle and coracoid process that followed the exact course of the coracoclavicular ligament and represented heterotopic ossification or myositis ossificans traumatica. This case has another distinctive feature, however: the examining orthopedist noticed a ridgelike or barlike ossification at the superior border of the right scapula (arrow in Fig. 5.3 c), which he could not identify. That feature was most likely a congenital (variant) ossification of the transverse scapular ligament, which shows a familial occurrence (Giordano 1962, cited in Freyschmidt’s “Köhler/Zimmer” 2001).17 , 41

Final Diagnosis
Posttraumatic myositis ossificans in the lateral portions of the trapezius muscle and surrounding an area of acro-osteolysis (avascular necrosis) at the peripheral end of the clavicle.
Comments
Linking together the three key radiologic findings in this case (soft-tissue ossifications in the lateral portion of the trapezius and around the peripheral end of the clavicle, plus acro-osteolysis at the peripheral end of the clavicle) based on their topographic relationship to one another and to the patient’s history is sufficient to identify this condition as myositis ossificans and distinguish it from an os omovertebrale.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


