5.2 Scapula
5.2.1 Case 83 (Fig. 5.9)

Case description
Referring physician: radiologist.
Prior history and clinical question: A 67-year-old man with prostate cancer underwent a staging whole-body bone scan (Fig. 5.9 b) which showed increased uptake along the superior margin of the left scapula, extending from the superior angle into the acromion. A less pronounced area of intense uptake was also noted in the inferior angle. The corresponding radiograph (Fig. 5.9 a) showed enlargement of the superior margin and acromion with a coarsened trabecular pattern . Question: Is this an unusual presentation of metastasis or something else? On repeated questioning, the patient denied having any complaints.
Pathoanatomic Background of the Findings
There is definitely an active bone remodeling process that has led to enlargement and a coarsened trabecular pattern.
Assignment to a Possible Basic Entity
Normal variant or malformation?
No, there is no normal variant involving a structural transformation in the upper portions of the scapula.
Tumor?
No, the geometry of the changes (elongated pattern, not rounded, coarsened trabecular pattern) is not consistent with a tumor or metastasis.
Perfusion disorder?
No, there is no known precedent in this anatomic region, and a perfusion disorder would not explain the coarsened trabecular pattern.
Regressive change?
No, what is there in the upper scapular margin that could undergo degenerative changes? There are attachments for muscles and tendons in that area, but degenerative enthesiopathy would not cause such intense tracer uptake or radiographic coarsened trabecular pattern and enlargement with smooth outer margins. Degenerative enthesiopathy would be more likely to cause a rarefying or productive fibro-osteitis with jagged outer margins.
Synopsis and Discussion
All of the above considerations suggest an inflammatory, nonbacterial, chronic bone remodeling process. The lack of clinical manifestations excludes a purely reactive process as in psoriasis or pustulosis palmoplantaris (see Case 84). The only remaining inflammatory osseous process is Paget disease (osteitis deformans) in the active late lytic stage or intermediate stage, although this would be a very unusual site of occurrence (sites of predilection are the pelvis, femur, tibia, and skull). But rare sites of involvement by Paget disease generally occur in the polyostotic form, not in a monostotic form. Even so, the following findings in our case support this diagnosis:
Age of the patient. Most cases of Paget disease are diagnosed after about 60 years of age, although the disease may develop much earlier. The bone remodeling disorder spreads from the initial focus at a rate of approximately 1 cm/year.
The absence of any symptoms.
Typical elongated distribution of highly abnormal tracer uptake on bone scans. This is not characteristic of a metastasis.
Coarsened trabecular pattern and enlargement of the affected bone area.
We also attributed the small focus in the inferior angle (Fig. 5.9 b) to Paget disease based on radiographic findings. Further investigation was unnecessary. Serum alkaline phosphatase was only slightly elevated. Based on the international guidelines, treatment is not indicated.
Fig. 5.10 a–e illustrates another case of Paget disease in the scapula, though it is just one of many lesions. This rare site of occurrence is found almost exclusively in the polyostotic form. Additional foci were present in the spine, pelvis (Fig. 5.10 d), and left distal femur (Fig. 5.10 e). The 65-year-old man was virtually asymptomatic, and the findings were noted incidentally on a whole-body bone scan (Fig. 5.10 a, b). His serum alkaline phosphatase level was six times higher than normal. Note the elongated and/or diffuse pattern of tracer uptake in the scapula and pelvis, which is so typical of active Paget disease. Radiographs of the scapula (Fig. 5.10 c) and pelvis (Fig. 5.10 d) show a mixed to early, active sclerotic stage of disease, with the distal femur showing a late sclerotic, less active stage (Fig. 5.10 e). Other examples of Paget disease are presented in Case 8, Case 9, Case 12, Case 14, Case 46, Case 51, Case 107, and Case 140.

Final Diagnosis
Rare occurrence of Paget disease (osteitis deformans) in the scapula.
Comments
An elongated, continuous pattern of tracer uptake in an older patient generally signifies Paget disease.
5.2.2 Case 84 (Fig. 5.11)

Case description
Referral: self-referral by the patient.
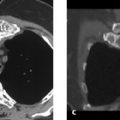
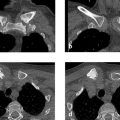
Prior history and clinical question: A 31-year-old woman had an approximately 2-year history of pustulosis palmoplantaris (PPP) (Fig. 5.11 f) with a fluctuating course. Symptoms began with pain in the left scapula, accompanied later by pain in the lower lumbar spine. A whole-body bone scan (Fig. 5.11 e) showed massive tracer uptake in the upper half of the left scapula with slightly increased uptake also noted around the manubrium sterni and in the L5 and S1 vertebrae. CT scans of the left scapula (Fig. 5.11 a, b) showed an extensive sclerotic process, which apparently originated from the periosteum, mainly on the costal side. MRI (Fig. 5.11 c, d) showed edema-like signal intensity, especially at paraosseous sites. A radiograph of the lumbar spine (not pictured here) showed predominantly marginal sclerosis in the lower portions of L5 and upper portions of S1. The intervertebral space was obliterated, and the upper and lower vertebral endplates showed slightly irregular margins. A biopsy was taken from the scapula and interpreted histologically as Garré osteomyelitis. Long-term antibiotic therapy was instituted at that point and was followed by some regression of the paraosseous edema-like signal, while clinical complaints persisted. Finally an orthopedist recommended a scapulectomy as a last resort. The patient found that very strange and asked us for a second opinion.
Radiologic Findings
The imaging findings are described above. It should be added that CT and MRI showed thinning and partial resorption of the scapular cortex, predominantly on the costal side. No destructive changes were found in the cancellous bone.
Location
Periosteal new bone formation and paraosseous edema-like signal were found predominantly on the costal side of the scapula, suggesting that the epicenter of the changes may lie at the enthesis, or zone of soft-tissue attachment to the bone (subscapularis muscle).
Pathoanatomic Background of the Findings
The findings indicate a mixed destructive and proliferative process whose distribution suggests a chronic active inflammation, very likely arising from entheses on the costal surface of the scapula.
Assignment to a Possible Basic Entity
Inflammation?
As stated above, the imaging findings are fully consistent with an inflammatory process. Since it appears to originate from the enthesis, the sclerosis in the scapula would correspond to a reactive inflammation (osteitis). An inflammatory process is also consistent with the changes in L5/S1 (spondylodiskitis) and the relatively subtle scintigraphic changes around the manubrium sterni,
Tumor?
No, there is no evidence of a tumor mass. When all pathologic findings are considered together, the scintigraphic and radiographic changes in the lumbar spine do not suggest a tumor such as lymphoma or osteosarcoma and are more consistent with an inflammatory process.
Synopsis and Discussion
The radiologic findings in the left scapula were apparently viewed in isolation and investigated by biopsy in the hope of establishing a clinically useful diagnosis. Histology indicated “Garré osteomyelitis,” a catch-all diagnosis for an indeterminate sclerosing osseous process. Garré published a report of his eponymic disease over 100 years ago (1893), and thus before the discovery of X-rays and the establishment of modern microbiology and antibiotic therapy, describing the condition as an acute onset of “fever and swelling of the extremities, pain and marked expansion of the soft tissues that suggests impending abscess formation.” He continued, “Instead, the infiltration gradually regresses while fever subsides more quickly, leaving behind only a variable degree of bone expansion while the patient makes gradual progress toward recovery.” He published all of this under the title “On Special Forms of Acute Infectious Osteomyelitis.”16 Garré was describing an acute infectious osteomyelitis that heals with bone expansion; he made no mention of sclerosis. That term stems from radiographic terminology used in relation to bone. We have no idea who, ignorant of the original paper, coined the term “Garré chronic sclerosing osteomyelitis,” or who then uncritically copied this altered term again and again over the years, but it would make an interesting subject for a dissertation on the history of medicine. From a modern-day perspective, osteomyelitis like that described by Garré would usually be called chronic osteomyelitis arising from an acute osteomyelitis that was treated improperly or too late, or was inherently resistant to antibiotics. Osteomyelitis associated with significant sclerosis, enlargement of the affected bone area, and mild, nonacute clinical symptoms is known as plasma cell osteomyelitis or a Brodie abscess. This differs from reactive forms of osteitis, which are not the same as osteomyelitis because they do not originate from bone marrow due to bacterial colonization. They are reactive processes resulting from an autoimmune disorder, for example, or from an enthesitis like that occurring in seronegative spondyloarthritis.
In the present case, the scapular change was just one manifestation of a systemic disease: pustular arthro-osteitis or enthesio-osteitis (PAO, PEO), known also as SAPHO, see Case 40. This is indicated by the following findings:
Clinical presence of pustulosis palmoplantaris (PPP) accompanied by pain in the left scapula and later in the lumbar spine
Oligolocular pattern of increased uptake on the whole-body bone scan
Periosteal enthesitic new bone formation and associated osteitis on CT scans
Paraosseous edema-like signal on MRI
Spondylodiscitic changes in L5/S1
These findings are sufficient to make a diagnosis of PAO or PEO and initiate treatment with anti-inflammatory and/or immune-modulating therapy; biopsy is unnecessary. It is important to recognize that pustulosis palmoplantaris is a variant of psoriasis and that psoriasis is not limited to the skin but is a systemic disease that may produce musculoskeletal involvement, cardiovascular changes (hypertension, coronary heart disease), etc. When anti-inflammatory and immune-modulating therapy was instituted in the present case, along with local treatment of the pustulosis palmoplantaris, the clinical and radiologic findings in our patient showed substantial improvement.
For comparison, Fig. 5.12 illustrates the case of a child with an osteosarcoma in the scapula. The dominant radiographic finding was sclerosis (Fig. 5.12 a) while CT (Fig. 5.12 b) showed fine destructive foci in the scapula with an extensive paraosseous tissue component and spiculations. Sclerosis results from ossification of the osteoid matrix formed by the tumor cells. The destructive mass lesion and demonstrable matrix ossification clearly distinguish the radiologic features of this case from the case in Fig. 5.11.

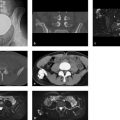
Another case of PAO or PEO, in a 54-year-old woman, is illustrated in Fig. 5.13 a–f. The unusual feature of this case is the presence of small cavities that contain sequestra, which are suggestive of infectious osteomyelitis (Fig. 5.13 b, d, e). But the whole-body bone scan showed a bull’s head sign in the sternoclavicular region (Fig. 5.13 c) and the patient had classic PPP (Fig. 5.13 f). These findings were diagnostic, eliminating the need for biopsy. Treatment consisted of immunomodulating therapy with methotrexate, and later cyclosporine, and by 2 years the previously pain-wracked patient was free of complaints. On our advice she later quit smoking, which her dermatologist believed had triggered and/or perpetuated the PPP. A radiologic follow-up at 10 years showed only residual sclerosis of the scapula.

Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


