5.4 Sternum
5.4.1 Case 95 (Fig. 5.35)

Case description
Referring physician: This case was kindly furnished to us by Prof. Dr. J. Schäfer, University of Tübingen.
Prior history and clinical question: A 14-year-old boy presented with pain in the lower sternum.
Radiologic Findings
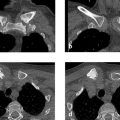
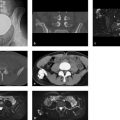
The CT images in Fig. 5.35 a–d demonstrate a punched-out defect in the left upper portions of the third segment of the body of the sternum. The attenuation values in the lesion range from 92 to 163 HU. The cortex is partially destroyed. MRI after IV contrast administration shows only moderate enhancement (Fig. 5.35 e). Diffuse hyperintensity is noted throughout the third sternal segment and in the lower portions of the second segment. Definite matrix calcification is not demonstrable by CT.
Pathoanatomic Background of the Findings
Findings indicate a solid destructive process that is moderately perfused but has incited a significant proton-rich perifocal reaction.
Assignment to a Possible Basic Entity
Normal variant or malformation?
No known precedents. Clinical manifestations and MRI findings are also inconsistent with a normal variant or malformation.
Trauma?
No trauma history.
Inflammation?
No clinical manifestations, and imaging shows no evidence of an abscess or paraosseous edema.
Tumor?
Yes, but what kind? Primary bone tumors are extremely rare in the sternum. The present case shows no matrix mineralization that might indicate a bone-forming or cartilage-forming tumor. The marked edema-like signal surrounding the destructive process could signify an osteoid osteoma, osteoblastoma, or perhaps even a chondroblastoma. The marked perifocal reaction is not characteristic of eosinophilic granuloma (Langerhans-cell histiocytosis), though apparently it may occur (see Fig. 4.12 in Case 55) due to local bone weakening or destruction. All in all, a benign tumor appears more likely than a malignancy owing to the apparent absence of spread to surrounding structures. The etiology in this case can be established only by histology; afterward the radiologist may consider the histologic diagnosis to be plausible or implausible, and the latter conclusion should prompt further evaluation of the case.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


