7.1 Equivocal MRI Findings
7.1.1 Case 128 (Fig. 7.1)

Case description
Referring physician: radiologist.
Prior history and clinical question: A 25-year-old woman sustained a twisting injury and was referred for MRI of the right knee joint. Signal anomalies were noted chiefly in the distal femoral metadiaphysis, raising a broad range of diagnostic possibilities.
Radiologic Findings
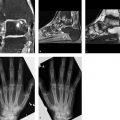
On T1-weighted (T1w) MRI, the imaged portions of the femur and tibia show scattered spots of relatively low signal intensity (Fig. 7.1 a, b), which appear bright in the water-sensitive sequence (Fig. 7.1 c). The spots enhance after intravenous (IV) contrast administration (Fig. 7.1 d). Similar changes were found on the contralateral side.
Location
All the findings are located in the medullary cavity of the diametaphysis while sparing the epiphyses.
Pathoanatomic Background of the Findings
The foci must have a moderately high proton density and must have a sufficient vascular supply based on their enhancement characteristics. They could be aggregates of normal but heterotopic bone marrow cells, or myeloproliferative lesions such as mastocytosis or malignant lymphoma.
Assignment to a Possible Basic Entity
Normal variant or malformation?
Possibly. Islands of bone marrow in medullary cavities containing mostly fatty marrow may occur in the long bones of healthy individuals, especially women. Some persons, currently healthy, may also have a prior history of one or more episodes of significant blood loss or heavy menstruation.
Inflammation?
No clinical manifestations.
Tumor or tumorlike lesion?
Yes, in principle, such as localized non-Hodgkin lymphoma, plasmacytoma, etc.
Synopsis and Discussion
Since the lesions were detected incidentally during knee MRI in a clinically healthy young woman, the spotty areas of altered signal intensity in the medullary cavity should be classified as an incidental finding or normal variant. This is even more likely when the same changes are found on the opposite side. The referring physician should be told, however, that a clinical examination (liver, spleen, and lymph nodes) and blood count are necessary to exclude an incipient hematologic disease. There is no need, however, to alarm the patient or referring physician.
Finally, it should be mentioned that islands of bone marrow in fat-containing diametaphyseal segments of long bones may not only form in the setting of increased hematopoiesis, for whatever reason, but may also occur physiologically during the conversion of red bone marrow to fatty marrow at about 20 years of age and then disappear completely by about 24 years of age. Apparently this process does not occur in some individuals, however, with the result that islands of bone marrow are still detectable for years or even for life.
Final Diagnosis
Islands of red marrow detected incidentally in the distal femoral metadiaphyses.
Comments
Islands of altered MRI signal intensity (hypointense on T1w images, hyperintense on T2w and STIR images, enhancing after contrast administration) in the distal femoral metadiaphysis should be considered a normal variant in otherwise healthy individuals.
7.1.2 Case 129 (Fig. 7.2)

Case description
Referral: parents of the patient.
Prior history and clinical question: A 6-year-old girl complained of exercise-related pain in her left proximal femur. Her parents stated that she also had several episodes of fever (about 38°C) in recent weeks. MRI of the left thigh raised suspicion of an eosinophilic granuloma or another tumor “that could not be ruled out.” Repeat scans 2 weeks later showed no change, and biopsy was recommended. A radiograph (Fig. 7.2 b) taken at the time of initial MRI appeared normal.
Radiologic Findings
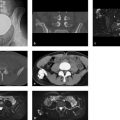
Both initial MRI (Fig. 7.2 a) and the follow-up series (Fig. 7.2 c, d) demonstrate a predominantly medial area of edema-like signal in the middle third of the left femoral shaft. A linear hyperintensity is visible along the medial cortex.
Location
The above MRI findings are arranged eccentrically about the medial side of the femoral cortex, so the cortex may be their epicenter. This suggests that the process does not originate from the bone marrow or medullary cavity (compare with Case 130).
Pathoanatomic Background of the Findings
As noted under Location, a primary process arising from the medullary cavity (Ewing sarcoma, eosinophilic granuloma, osteomyelitis) appears unlikely. Edema-like signal changes with a cortical epicenter may have a traumatic etiology.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


