7.4 Changes with Mixed Features
7.4.1 Case 150 (Fig. 7.37)

Case description
Referring physician: orthopedist.
Prior history and clinical question: A 10-year-old boy was kicked in the right knee while playing soccer. Afterward he complained of anteromedial knee pain and walked with a limp. He was an avid athlete and denied any previous joint complaints. Clinical examination 4 days later showed no external bruising and normal knee function. MRI was ordered “as a precaution.”
Radiologic Findings
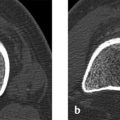
On the T1w images in Fig. 7.37 a–c, the bony portion of the lateral femoral condyle has a smaller volume posteriorly than the medial condyle, and the epiphyseal cartilage layer is very thick. The articular-sided border of the ossified lateral femoral condyle has a proximal convex outline and a somewhat jagged appearance. The water-sensitive images in Fig. 7.37 d–h show no evidence of edema-like signal in the lateral condyle. There is no visible bony element congruent with the apparent condylar defect.
Location
The apparent volume defect is located in the posterior bony portion of the lateral femoral condyle.
Pathoanatomic Background of the Findings
The ossification center of the distal femoral epiphysis (i.e., of the condyles) may have different medial and lateral calibers during growth and may present irregular contours. Asymmetries are not necessarily abnormal, therefore.
Assignment to a Possible Basic Entity
Normal variant or malformation?
Yes. As noted above, the medial and lateral portions of the ossification center of the distal femoral epiphysis may have different volumes during growth and may show corresponding volume changes in the overlying articular cartilage.59 A normal variant is suggested by the negative history and by the absence of complaints at the time of clinical examination, with a normal gait and normal function tests. None of the MRI sequences shows any evidence of a pathologic process such as edema-like signal in the subchondral region of the medial femoral condyle.
Synopsis and Discussion
The apparent posterior depression in the ossification center of the lateral femoral condyle in this case prompted discussion about the possibility of osteochondritis dissecans. It was tempting, of course, to interpret the jagged bony depression as a defect due to osteonecrosis. But a matching fragment could not be found in the bone or in the adjacent joint. The cartilage overlying the depression does show compensatory thickening but otherwise appears completely healthy by MRI. There are no typical signs of osteochondritis dissecans such as edema-like signal in the adjacent bone or a hyperintense subchondral line or zone of demarcation. Moreover, the patient had no clinical manifestations and a negative prior history. By 1 year after initial imaging, the boy was completely free of complaints and was fully able to participate in sports. Since the advent of MRI in the diagnosis of osteochondritis dissecans, we have repeatedly observed similar findings that “resolved” over a period of months or years with no clinical sequelae.17 Regardless of this, irregular contours and volume discrepancies between the medial and lateral portions of the distal ossification center, including multiple centers, are not unusual.
Final Diagnosis
Normal variant in the ossification of the distal lateral femoral epiphysis.
Comments
Variations in the volume and contours of ossification centers are likely to occur during skeletal growth. These normal variants require differentiation from osteonecrosis, especially osteochondritis dissecans.
7.4.2 Case 151 (Fig. 7.38)

Case description
Referring physician: pediatric orthopedist.
Prior history and clinical question: A 1-year-old overweight child was found to have an increasing but painless varus deformity of the left knee and lower leg.
Radiologic Findings
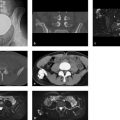
Radiographs show a deep, medial depression with a sclerotic margin at the proximal meta-diaphyseal junction of the left tibia (Fig. 7.38 a). The cortex distal to the depression is markedly thickened. Varus angulation of the tibia is also noted.
Location
The depression is located precisely at the insertion of the pes anserinus—the conjoined tendon of the sartorius, semitendinosus, and gracilis muscles.
Pathoanatomic Background of the Findings
The location of the depression at the pes anserinus insertion which is responsible for the varus deformity suggests that we are dealing with stress-induced bone resorption similar to a fibrous metaphyseal defect (e.g., at the insertion of the gastrocnemius heads).
Assignment to a Possible Basic Entity
Normal variant or malformation?
No, because we are dealing with an acquired, progressive change that became clinically apparent during the first year of life.
Trauma?
Yes. As mentioned above, the deformity was apparently a stress-induced change that developed when the somewhat overweight child learned to walk. The insertion of the pes anserinus is an enthesis, which appears to be very sensitive to overuse.
Inflammation?
No clinical manifestations.
Tumor or tumorlike lesion?
The concave defect could perhaps have been caused by an adjacent soft-tissue tumor. But the above considerations are more indicative of a stress-induced change that mimics a tumor and thus belongs in the category of tumorlike lesions.
Synopsis and Discussion
The stress-related defect in the medial tibial metaphysis is also known as focal fibrocartilaginous dysplasia. This term expresses the main histologic features of the lesion: the defect contains inactive fibrocytes and connective tissue with interspersed chondrocytes, which are elements of a fibrocartilaginous enthesis, except that the tissue is richer in collagen fibers and connective tissue than normal. The marked cortical thickening distal to the defect also suggests a stress-induced change. Similar to Blount disease (see Fig. 7.39), the dysplasia occurs in small children learning to walk and apparently results from unaccustomed stress on the pes anserinus enthesis. Unlike Blount disease, it is typically associated with unilateral tibia vara. The stress-induced change resolves spontaneously over the next 2 to 3 years, as demonstrated by the follow-up images (Fig. 7.38 b, c). Surgical correction and biopsy are both obsolete. As one would expect, MRI shows a mixed, predominantly hypointense signal pattern in the soft-tissue lesion.

Fig. 7.39 illustrates a typical case of Blount disease, a growth disturbance characterized by bilateral varus bowing of the tibiae. It is observed in children and adolescents but, at least in the cases we have seen, appears to begin during the first year of life, affecting predominantly overweight children who learn to walk too early. Known also as “toddler’s disease,” it apparently results from a disturbance in the proliferation of growth cartilage in the medial proximal growth plates of the tibiae, leading to abnormal longitudinal growth on the medial side and varus bowing. Later, disturbances may also occur in the medial femoral growth plates. Unlike focal fibrocartilaginous dysplasia, the disease is progressive and does require surgical correction. A genetic predisposition is unknown. Radiographs typically show beaking of the medial tibial metaphyses with genu varum. In the case shown, similar changes are already apparent in the medial femoral metaphyses.
Final Diagnosis
Focal fibrocartilaginous dysplasia due to stress-induced enthesiopathy at the insertion of the pes anserinus.
Comments
The location of a lesion is often crucial for the correct interpretation of a radiologic abnormality.
7.4.3 Case 152 (Fig. 7.40)

Case description
Referring physician: radiologist.
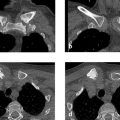
Prior history and clinical question: A 14-year-old boy presented with an extreme valgus deformity of the right knee with pain on weight-bearing. When we saw him, we elicited more details on his history and learned that he was a goalkeeper in his soccer team. When diving for a ball, he had a habit of landing on the ground with his right knee. He participated in soccer practice at least four times a week. A radiograph of the right knee joint showed extreme valgus deformity with maximum angulation at the growth plate, posterior slippage of the distal femoral epiphysis, and marked sclerotic changes about the lateral growth plate and over the bone surface. These sclerotic changes were considered suspicious for osteosarcoma.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


