Abstract
Spinal cord lipomas concurrent with spinal arteriovenous fistulas (SAVFs) are rare, and their natural history and optimal treatment remain unclear. We report the case of a 44-year-old woman with a history of surgical intervention at 2 months of age for myelomeningocele, with the possibility of lipmyelomingocele based on the surgical history, who presented with progressive paralysis and paresthesia in both lower extremities over 3 years. She was diagnosed with an SAVF concurrent with a congenital spinal lipoma, and transarterial embolization was performed after confirming the absence of neurological symptoms during a provocation test. Postoperative imaging showed reduced T2-weighted high-intensity signals in the spinal cord, and 3 months after the procedure, her neurological symptoms improved significantly, allowing her to transition from nonambulatory wheelchair dependence to ambulation with a double cane. This case highlights the need for detailed imaging and vascular evaluation in patients with spinal lipomas and SAVFs, especially in cases involving the filum terminale type, which is closely associated with the anterior spinal artery. Proximal occlusion may occur if feeders have multiple branches or a long distance to the drainer, increasing the risk of incomplete treatment. A provocation test before embolization can enhance both safety and efficacy.
Introduction
Spinal lipomas concurrent with spinal arteriovenous fistula (SAVF) are rare, and only a few cases have been reported to date. In this report, the patient experienced neurological symptoms exacerbated by a spinal arteriovenous shunt, which was likely attributable to a congenital spinal lipoma. Herein, we report a favorable outcome achieved through transarterial embolization (TAE) with endovascular treatment and present a review of literature on similar cases. The research within our submission has been approved by the ethics institutional review board of our hospital.
Case presentation
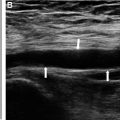
A 44-year-old woman with a history of myelomeningocele surgery at 2 months of age, with the possibility of lipomyelomenigocele based on the surgical history, presented with bladder and bowel dysfunction managed with self-catheterization and laxatives. Three years ago, she developed paresthesia in both lower limbs, which progressed to her upper limbs 2 months prior to presentation. Her gait disturbance worsened, rendering her wheelchair-dependent. Following detailed imaging and neurological assessment, she was referred to our hospital by her primary care physician for evaluation of her progressing symptoms. Neurological findings upon presentation to our hospital revealed muscle weakness of her lower limbs with pain and paresthesia with accompanying dysesthesia. The manual muscle testing (MMT) of the lower limbs showed the following results: iliopsoas 2/2, quadriceps femoris 3/3, tibialis anterior 0/0, extensor hallucis longus 2/2, flexor hallucis longus 2/2, and gastrocnemius 0/0. The Aminoff–Logue disability scales for gait and micturition were G5 and M3, respectively. Physical findings included a surgical scar on the lumbar region present since infancy, a bulging lipoma in the same region, and a sacral dimple ( Fig. 1 A, B). T2WI of spinal MR imaging revealed intramedullary high-intensity signal changes from the level of the sixth thoracic vertebra to conus medullaris as well as a flow void around the spinal cord ( Fig. 1 C). Presence of a lipoma extending from her buttocks to the first sacral vertebra level of the spinal canal and continuity with the spinal cord is observed at the same elevation ( Fig. 1 D). T1WI of MR imaging at the level of the first sacral vertebra showed the lipoma was located of the dorsal side of the spinal cord ( Fig. 1 E). There was contiguous alignment with the spinal lipoma and conus medullaris, but the cauda equina was not observed ( Fig. 1 F). Contrast-enhanced CT and DSA revealed first and third sacral artery branching from the left lateral sacral artery, and median sacral artery, formed a shunt onto the spinal lipoma, and a draining vein ascending ventral to the spinal cord ( Fig. 2 A-F). The third sacral artery exhibited a vascular architecture overlying the spinal lipoma. It divided into 3 major branches, each forming distinct shunt points. These branches ultimately drained into the common vein that was previously identified and ascended on the ventral side of the spinal cord ( Fig. 2 G-H). Based on these findings, we diagnosed SAVF with a shunt overlying the spinal lipoma and contributed mainly by a branch from the left third sacral artery. After discussing the treatment plan with the spinal surgery group, the patient opted for endovascular treatment due to the inherent high risk of damaging spinal nerve fibers traversing within the lipoma during an open surgery.


Endovascular treatment was performed through a puncture of the right femoral artery under local anesthesia, and the Guiding catheter (Axcelguide Guiding System 4Fr 75 cm Mori-1, Medikit, Tokyo, Japan) was inserted. We used a microguidewire (Chikai10 Micro Guide Wire 0.010’’ 200cm, ASAHI INTECC, Aichi, Japan) to guide and an intermediate catheter (Guidepost 3.2/3.4Fr 120cm, Tokai Medical Products, Aichi, Japan) to support the microcatheter. The intermediate catheter was guided to the left third sacral artery, and a provocation test with 10 mg of lidocaine was performed to confirm that no neurological symptoms had developed. A flow-guide microcatheter (Marathon Flow Directed catheter 2.7/1.5Fr, 165cm, Medtronic, Minnesota, USA) was guided into one of the feeders from the left third sacral artery, and N-butyl cyanoacrylate (NBCA) liquid adhesive (Histoacryl, B.Braun, Melsungen, Germany) diluted to 20% with ethyl ester of iodinated poppy-seed oil fatty acid (Lipiodol, Guerbet Japan, Tokyo, Japan) was used for TAE. Injection of 0.09 ml NBCA resulted in partial feeder embolization due to the backflow. A more distal feeder was selected using a flow-direct microcatheter (DeFrictor Nano Flow Directed catheter 2.2/1.3Fr 165 cm, Medico’s Hirata, Osaka, Japan), and TAE was performed again with 20% NBCA. TAE was performed with 0.33 ml of NBCA to achieve partial embolization, and the embolization was terminated as NBCA reflux was observed reaching up to the third sacral artery ( Fig. 2 I). Immediately after surgery, the patient experienced improvement in ankle paralysis and pain caused by dysesthesia but, since the treatment was limited to arterial embolization, there was a risk of recurrence of the AVF and the plan was to follow up with imaging studies.
T2WI of MR imaging on the second postoperative day revealed a flow void around the spinal cord and weakening of the intramedullary T2 high-intensity signal ( Fig. 3 A, B). Contrast-enhanced CT on the third postoperative day showed decreased venous drainage through the fistula; however, residual blood flow persisted and a feeding artery from the left first sacral artery was evident ( Fig. 3 C, D). The patient was retreated 9 days postoperatively. Similar to the first procedure, angiography was performed under local anesthesia through a puncture of the right femoral artery. This confirmed the presence of an AVF arising from the left first sacral artery, which was not observed and became apparent in the previous procedure. A shunt was formed from the left lateral aspect of the artery to the base of the lipoma and draining into the ventral vein ascending from the right lateral side ( Fig. 4 A, B). The flow-direct catheter was guided to the S1 radicular artery at first sacral foramen level ( Fig. 4 C). Embolization was performed with 16.7% NBCA because of the large distance between the catheter and recipient vein. NBCA (0.13 ml) was injected into the fistulous tract, but extravasation occurred near the first sacral foramen at the end of the procedure due to continuous pressure infusion ( Fig. 4 D). The extravasation site was immediately embolized with additional NBCA infusion, and no symptoms occurred during this procedure.


Two days after retreatment, T2WI of MR imaging confirmed the disappearance of the flow void and intramedullary high-intensity signal ( Fig. 4 E). CT angiography revealed casts of NBCA in the first sacral artery and the partially in the recipient vein, confirming that the vein had lost its angiographical delineation ( Fig. 4 F, G). The postoperative evaluation of the lower limb MMT revealed the following improvements: iliopsoas 4/2, quadriceps femoris 4/4, tibialis anterior 1/1, and gastrocnemius 0/0. Additionally, the pain level associated with dysesthesia improved to one-tenth of the preoperative level. The patient showed clinical improvement and was transferred to a rehabilitation hospital on the 17th postoperative day. Three months after discharge from our hospital, T2WI of MR imaging showed decreased volume of spinal lipoma and findings of attenuated T2 high-intensity signal changes in the spinal cord ( Fig. 4 H). The patient showed improvement in ambulation from preoperative wheelchair level to walking with a double cane; moreover, the patient advanced from G5 to G4 on the Aminoff–Logue scale, although abnormal sensation persisted. Since only partial casts were identified on the drainer side, the patient will continue to be followed on an outpatient basis for possible AVF recurrence.
Discussion
Spinal lipoma is a developmental abnormality due to infiltrated fatty tissue during neural tube formation, occurring in approximately one in 4000 births, with a male-to-female ratio of approximately 1:1.5 [ ]. In 1982, Chapman et al. classified spinal lipomas into 3 types: dorsal type, caudal type, and transitional type. Further, in 2001, Arai et al. added the filar type and lipomyelomenigocele type, expanding the classification to 5 types [ ]. Pang et al. placed complex and challenging cases that did not follow the criteria for either dorsal or transitional type in a separate category known as chaotic type [ , ]. Recently, Morota et al. proposed a new classification system for spinal lipomas based on embryological stages. Based on Morota’s classification, type 1 refers to a primary neural tube formation failure, and the key feature is that the conus medullaris is formed caudal or ventral to the lipoma. Therefore, a case in which a lipoma extends from the dorsal to the caudal side of the conus medullaris, if conus medullaris is formed, it is classified as a transitional type based on conventional classification and is classified as type 1 based on Morota’s classification. The current case meets the criteria for being type 1 according to Morota’s classification [ ].
Spinal arteriovenous fistulas (AVFs) have historically been classified based on angiographic findings and surgical observations, such as the location and morphology of the shunt [ ]. However, no standardized classification system currently exists. Additionally, no classification has been proposed for spinal AVFs coexisting with tumors or spinal lipomas. Myelopathy is generally a chronic and progressive condition due to impaired venous perfusion. It can lead to acute spinal cord paralysis due to intramedullary or subarachnoid hemorrhage. Concomitant cases of SAVM and spinal lipoma are rare, with only 23 cases reported since 1989, when Djindjian et al. first reported the combined case [ ]. However, their natural history, pathogenesis, classification and treatment strategies are yet to be established. SAVFs may also occur below the conus medullaris without complications of spinal lipoma. Hong et al. reported 3 types of AVFs: filum terminale AVF, spinal dural AVF, and radicular AVF but, did not classify the cases associated with lipoma [ ]. In the present case, we reviewed 24 previously reported cases of spinal lipomas complicated with SAVF, including the present case ( Table 1 ) [ ].
Related posts:
 A rare and life-threatening case of spontaneous hemopneumothorax presenting with severe hemodynamic instability
A rare and life-threatening case of spontaneous hemopneumothorax presenting with severe hemodynamic instability
 A very rare case of ileocolic and appendiceal intussusception with acute appendicitis
A very rare case of ileocolic and appendiceal intussusception with acute appendicitis
 Hepatic and extra-hepatic hydatid cysts: A case series of radiological and clinical insights
Hepatic and extra-hepatic hydatid cysts: A case series of radiological and clinical insights
 Mid-term follow-up of a fractured flow diverter in the internal carotid artery
Mid-term follow-up of a fractured flow diverter in the internal carotid artery
 An atypical multiple autoimmune syndrome: A case report including myocarditis
An atypical multiple autoimmune syndrome: A case report including myocarditis
 Successful ilio-femoral-popliteal venous aspiration thrombectomy using a 12 French system in a pediatric patient
Successful ilio-femoral-popliteal venous aspiration thrombectomy using a 12 French system in a pediatric patient
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


