Abstract
Epididymal leiomyoma is an exceptionally rare benign neoplasm originating from the smooth muscle of the epididymis. Due to its rarity and nonspecific clinical presentation, it poses significant diagnostic challenges. This case report describes a 50-year-old male who presented with a painless, progressively enlarging swelling in the right hemiscrotum over 3 years. Physical examination revealed a firm, nontender, well-demarcated swelling separate from the right testis. The initial ultrasound demonstrated a heterogeneous hyperechoic lesion with minimal vascularity on Doppler imaging, and a mild hydrocele was also noted. Further evaluation using contrast-enhanced CT revealed a heterogeneously enhancing paratesticular mass arising from the epididymis, with the right testis unaffected. The patient underwent a right-sided high inguinal orchidectomy for definitive management. Histopathological examination confirmed the diagnosis of leiomyoma, revealing interlacing fascicles of spindle cells characteristic of smooth muscle origin without evidence of malignancy. The postoperative period was uneventful, and the patient was discharged with instructions for regular follow-up. This case underscores the importance of a comprehensive diagnostic approach combining advanced imaging techniques and histopathological evaluation to accurately diagnose rare epididymal tumors. Surgical excision not only provides a therapeutic resolution but also facilitates definitive diagnosis. Awareness of such rare entities is critical for clinicians to differentiate them from other paratesticular masses, particularly malignant ones. This report adds to the limited literature on epididymal leiomyoma and highlights the need for multidisciplinary collaboration in managing such rare cases.
Background
Leiomyomas are benign mesenchymal tumors originating from smooth muscle cells and are most frequently encountered in organs with abundant smooth muscle, such as the uterus, gastrointestinal tract, and skin [ ]. Their occurrence in the epididymis, a structure predominantly composed of connective tissue and ductal epithelium, is exceedingly rare, accounting for less than 0.5% of all paratesticular tumors [ , ]. Due to their rarity, epididymal leiomyomas often pose diagnostic challenges and may be misdiagnosed as other benign or malignant paratesticular masses, such as lipomas, adenomatoid tumors, or sarcomas [ ].
Clinically, epididymal leiomyomas typically present as a painless, slow-growing scrotal mass often discovered incidentally. Symptoms are generally nonspecific, and patients may remain asymptomatic for prolonged periods, as in the current case, where the lesion remained undiagnosed for 3 years. These tumors are benign, but accurate diagnosis is crucial to differentiate them from malignant lesions, which require more aggressive management [ , ].
Diagnostic imaging plays a pivotal role in evaluating scrotal and paratesticular masses. Ultrasound is the first-line imaging modality, given its accessibility, cost-effectiveness, and ability to characterize the internal architecture of scrotal lesions [ ]. On Doppler imaging, epididymal leiomyomas are typically visualized as well-defined, hypoechoic, or heterogeneous masses with low vascularity. However, findings are often nonspecific, necessitating advanced imaging techniques for further evaluation. Contrast-enhanced computed tomography (CT) and magnetic resonance imaging (MRI) provide additional anatomical and vascular information, aiding in preoperative planning and differentiation of benign from malignant lesions [ ].
Histopathological examination remains the cornerstone of definitive diagnosis. Leiomyomas are composed of interlacing fascicles of spindle cells with eosinophilic cytoplasm and elongated nuclei, characteristic of smooth muscle origin. Immunohistochemistry can further confirm the diagnosis by demonstrating smooth muscle markers, such as smooth muscle actin (SMA) and desmin [ ]. Surgical excision is the treatment for epididymal leiomyomas, as it allows both diagnostic confirmation and therapeutic resolution. A high inguinal orchidectomy is often performed to ensure complete excision and to rule out malignancy. The prognosis is excellent, with minimal risk of recurrence or complications following surgery. However, the rarity of this condition necessitates reporting such cases to enhance clinical understanding and guide future management [ ].
Case presentation
A 50-year-old male presented to the surgical outpatient department with a history of swelling in the right hemiscrotum for the past 3 years. The swelling was insidious in onset and had progressively increased in size over time. The patient denied experiencing any associated pain, discharge, redness, trauma, or fever. He did not report any urinary symptoms or systemic complaints. No significant medical, surgical, or family history was relevant to his presentation.
On physical examination, the swelling was confined to the right hemiscrotum. It was firm in consistency, nontender, and separate from the right testis, which was palpable and normal in size and texture. There were no signs of inflammation, and the overlying skin appeared unremarkable. The left hemiscrotum, including the testis and epididymis, was normal.
To further evaluate the swelling, an ultrasound of the scrotum was performed. It revealed a heterogeneously hyperechoic, well-defined solid lesion measuring approximately 6.7 × 6.3 cm in the right paratesticular region. The lesion demonstrated a characteristic whorl pattern and showed minimal vascularity on Doppler imaging. A mild hydrocele was also observed in the right hemiscrotum, while the right testis was noted to be separate from the lesion. The left testis appeared normal in structure and echogenicity Figure 1 .

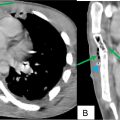
Subsequently, a contrast-enhanced CT (CECT) scan of the pelvis was performed to further delineate the lesion and evaluate its relationship with surrounding structures. The scan revealed a heterogeneously enhancing soft tissue mass lesion within the right scrotal sac from the epididymis. The lesion was separate from the right testis, which was normal in appearance. Mild hydrocele was confirmed on the imaging. The left testis was unremarkable Figure 2 .

Related posts:
 Breast cancer with medullary features shows a fast and plateau enhancement pattern on magnetic resonance images: A case report
Breast cancer with medullary features shows a fast and plateau enhancement pattern on magnetic resonance images: A case report
 A rare and life-threatening case of spontaneous hemopneumothorax presenting with severe hemodynamic instability
A rare and life-threatening case of spontaneous hemopneumothorax presenting with severe hemodynamic instability
 Primary sternal osteomyelitis in an immunocompetent adolescent
Primary sternal osteomyelitis in an immunocompetent adolescent
 Avascular necrosis of lateral femoral condyle in a middle-aged woman from central India
Avascular necrosis of lateral femoral condyle in a middle-aged woman from central India
 A very rare case of ileocolic and appendiceal intussusception with acute appendicitis
A very rare case of ileocolic and appendiceal intussusception with acute appendicitis
 An incidental finding of an ectopic intrauterine device (IUD) in the urinary bladder wall in a female presented with missed abortion
An incidental finding of an ectopic intrauterine device (IUD) in the urinary bladder wall in a female presented with missed abortion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


