Abstract
Muscular cysticercosis is a rare infection caused by Taenia solium , typically identified incidentally during imaging for unrelated symptoms. This report describes the case of a 60-year-old male who presented with a 6-month history of dull abdominal pain and swelling in the left inguinal region. The abdominal pain, initially localized to the right hypochondrium, gradually radiated to the left hypochondrium, with no known triggers or alleviating factors. The left inguinal swelling was nontender, soft, and exhibited a cough impulse. The patient had a medical history of nonmuscle invasive low-grade papillary urothelial carcinoma, treated with transurethral resection of bladder tumor (TURBT) and intravesical BCG therapy. Radiological investigations, including contrast-enhanced computed tomography (CECT) of the abdomen and pelvis, revealed multiple calcified granulomas measuring 9-10 mm in the left diaphragm, bilateral intercostal muscles, left erector muscle, right psoas muscle, and bilateral gluteal and thigh muscles. These findings were consistent with muscular cysticercosis. An X-ray AP view of the bilateral upper thighs corroborated these findings, showing multiple radiopaque soft tissue lesions in the bilateral gluteal and thigh muscles. A hypodense lesion in the spleen, measuring 12 × 8 mm, was also observed, with no evidence of malignancy. This case underscores the importance of thorough diagnostic evaluation in endemic regions, where parasitic infections such as cysticercosis may present atypically. While the patient’s primary complaints were not directly related to cysticercosis, the incidental findings emphasized the value of imaging in identifying and managing such conditions. Awareness and early recognition of muscular cysticercosis are crucial to prevent complications and guide appropriate management.
Background
Cysticercosis, caused by the larval stage of the tapeworm Taenia solium , is a significant parasitic disease with a global distribution but is predominantly endemic in regions with poor sanitation, where pig farming and consumption of undercooked pork are common [ ]. The life cycle of T. solium involves pigs as intermediate hosts and humans as definitive hosts. Humans can inadvertently become intermediate hosts by ingesting T. solium eggs through contaminated food, water, or direct fecal-oral transmission, developing cysticerci in tissues such as the brain, skeletal muscles, eyes, and subcutaneous tissue [ , ]. Among the various forms of cysticercosis, neurocysticercosis is the most studied due to its significant impact on public health, being a leading cause of epilepsy in endemic regions [ ]. In contrast, muscular cysticercosis is less frequently reported and often remains asymptomatic, discovered incidentally during imaging or surgical procedures. The pathophysiology involves the encystment of larvae in the musculature, which can result in localized inflammation, fibrosis, or calcification over time. Clinically, it may present as a painless or tender swelling, myositis, or calcified granulomas in chronic stages [ , ].
Radiological modalities play a crucial role in diagnosing muscular cysticercosis. X-rays can reveal radiopaque calcified lesions, while ultrasound and computed tomography (CT) provide detailed imaging of active and calcified cysts. Magnetic resonance imaging (MRI) is particularly valuable for differentiating cysticercosis from other soft-tissue pathologies [ ]. In endemic areas, characteristic imaging findings, such as “dot-in-hole” or calcified nodules, warrant a high index of suspicion for cysticercosis [ ]. Management of muscular cysticercosis depends on symptomatology. Asymptomatic cases often require no treatment, whereas symptomatic cases may benefit from antiparasitic therapy with albendazole or praziquantel, corticosteroids to mitigate inflammation, and symptomatic pain management [ , ]. Misdiagnosis can lead to unnecessary interventions, highlighting the importance of clinical awareness and accurate radiological interpretation. This report illustrates a rare case of muscular cysticercosis discovered incidentally during the evaluation of a patient with abdominal and inguinal symptoms. It underscores the significance of considering parasitic infections in endemic regions, particularly when atypical or incidental findings arise during imaging.
Case presentation
A 60-year-old male presented to the outpatient department with complaints of abdominal pain and a swelling in the left inguinal region, both persisting for the past 6 months. The abdominal pain initially began in the right hypochondrium, was insidious in onset, and progressively worsened over time. The pain was described as dull and aching, radiating to the left hypochondrium. The patient reported no aggravating or relieving factors. He also experienced intermittent episodes of vomiting but denied any association with specific food intake or other triggers.
The patient had no known history of systemic illnesses such as diabetes mellitus, tuberculosis, bronchial asthma, or hypertension. He reported a history of alcohol use but stated that he had stopped drinking a year before the presentation. His medical history included a diagnosis of nonmuscle invasive low-grade papillary urothelial carcinoma of the urinary bladder, for which he underwent transurethral resection of bladder tumor (TURBT) followed by 3 cycles of intravesical BCG therapy. There was no family history of similar complaints or significant illnesses.
On physical examination, the patient appeared well-nourished and in no apparent distress. Abdominal examination revealed a normal contour with the umbilicus midway between the xiphisternum and the symphysis pubis. There were no visible scars, pigmentation, or engorged veins. All abdominal quadrants moved symmetrically with respiration. On palpation, mild tenderness was noted in the right hypochondrium, but there were no signs of organomegaly, abdominal distension, guarding, or rigidity. Examination of the left inguinal region revealed a 3 × 2 cm swelling that was soft, nontender, and nonreducible, with a positive cough impulse. The overlying skin appeared normal without erythema, temperature changes, or visible veins. Bilateral testes were palpable and normal in size and texture.
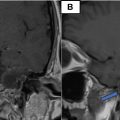
Imaging studies were performed to further evaluate the patient’s complaints. A CECT scan of the abdomen and pelvis revealed multiple calcified granulomas in the left diaphragm, bilateral intercostal muscles, left erector muscle, right psoas muscle, and bilateral gluteal and thigh muscles. Each granuloma measured approximately 9-10 mm, and the findings were consistent with muscular cysticercosis. Additionally, a hypodense lesion measuring 12 × 8 mm was identified in the spleen, though it showed no signs of malignancy Figs. 1-4 . The liver, gallbladder, pancreas, kidneys, and other abdominal organs were normal in size and appearance, and no lymphadenopathy was observed. The skeletal structures displayed degenerative changes likely attributable to age.

Related posts:
 Breast cancer with medullary features shows a fast and plateau enhancement pattern on magnetic resonance images: A case report
Breast cancer with medullary features shows a fast and plateau enhancement pattern on magnetic resonance images: A case report
 A rare and life-threatening case of spontaneous hemopneumothorax presenting with severe hemodynamic instability
A rare and life-threatening case of spontaneous hemopneumothorax presenting with severe hemodynamic instability
 Avascular necrosis of lateral femoral condyle in a middle-aged woman from central India
Avascular necrosis of lateral femoral condyle in a middle-aged woman from central India
 A very rare case of ileocolic and appendiceal intussusception with acute appendicitis
A very rare case of ileocolic and appendiceal intussusception with acute appendicitis
 An incidental finding of an ectopic intrauterine device (IUD) in the urinary bladder wall in a female presented with missed abortion
An incidental finding of an ectopic intrauterine device (IUD) in the urinary bladder wall in a female presented with missed abortion
 Petrous apex epidermoid cyst: A rare case
Petrous apex epidermoid cyst: A rare case
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


