Abstract
Tuberculous cystitis is a rare manifestation of genito urinary tuberculosis (TB), often presenting with nonspecific urinary symptoms and mimicking bladder cancer. This report presents a case of a 60-year-old male with concurrent pulmonary tuberculosis and tuberculous cystitis. The patient underwent imaging and biopsy for evaluation of hematuria and systemic symptoms. Diagnostic modalities included ultrasound, computed tomography (CT) scan, and polymerase chain reaction (PCR) for Mycobacterium tuberculosis.Imaging revealed a sessile bladder mass with associated hydroureteronephrosis and peri‑vesical fat densification. Additional findings included a left apico-dorsal pulmonary lesion. Biopsy confirmed granulomatous inflammation with caseating necrosis in the bladder. PCR for tuberculosis was positive despite negatives putums mears. Tuberculous cystitis is a diagnostic challenge due to its mimicry of malignancy. This case emphasizes the importance of biopsy and PCR in confirming TB. The coexistence of pulmonary tuberculosis underscores the systemic nature of the disease. This case highlights the diagnostic complexities of extrapulmonary TB and underscores the necessity of thorough investigation in patients with hematuria and atypical imaging findings.
Introduction
Tuberculosis (TB) remains a significant global health challenge, with genitourinary tuberculosis accounting for approximately 15%-20% of extrapulmonary TB cases. Tuberculous cystitis, a manifestation of genitourinary TB, is rare and often presents with nonspecific symptoms such as hematuria, urinary frequency, and pelvic pain [ ]. The clinical and radiological findings frequently mimic bladder malignancies, leading to diagnostic delays [ ]. This report describes a rare case of tuberculous cystitis in a 60-year-old smoker, highlighting its association with pulmonary tuberculosis and the role of advanced diagnostics in confirming the diagnosis.
Case report
A 60-year-old male with a history of heavy smoking presented with microscopic hematuria, left iliac crest pain, and thoracic spine discomfort localized to T11 and T12. An initial ultrasound revealed a sessile bladder tumor measuring 3 cm, located near the left ureteral meatus, with associated left hydroureteronephrosis.
Computed tomography (CT) of the thorax, abdomen, and pelvis (TAP) showed:
- •
A thickened bladder wall, predominantly involving the left lateral wall, with moderate upstream hydroureteronephrosis and densification of the peri‑vesical fat.
- •
A thickened and enhanced premeatal ureter segment measuring 19 mm in length, without further upstream dilation.
- •
A hypo-functioning right kidney with significant atrophy.
- •
A left apico-dorsal cavitary pulmonary lesion measuring 18 x 18 mm, suspected of being infectious or neoplastic.
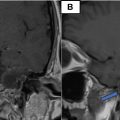
Biopsy of the bladder mass revealed granulomatous inflammation with multinucleated giantcells and caseating necrosis, consistent with tuberculosis. PCR testing for Mycobacterium tuberculosis on bladder tissue was positive, while sputumsmears were negative but PCR-positive Figs. 1 , 2 and 3 .

Related posts:
 Breast cancer with medullary features shows a fast and plateau enhancement pattern on magnetic resonance images: A case report
Breast cancer with medullary features shows a fast and plateau enhancement pattern on magnetic resonance images: A case report
 A rare and life-threatening case of spontaneous hemopneumothorax presenting with severe hemodynamic instability
A rare and life-threatening case of spontaneous hemopneumothorax presenting with severe hemodynamic instability
 Avascular necrosis of lateral femoral condyle in a middle-aged woman from central India
Avascular necrosis of lateral femoral condyle in a middle-aged woman from central India
 A very rare case of ileocolic and appendiceal intussusception with acute appendicitis
A very rare case of ileocolic and appendiceal intussusception with acute appendicitis
 Rare case of left epididymo-orchitis complicated by pampiniform plexus thrombosis: A case report
Rare case of left epididymo-orchitis complicated by pampiniform plexus thrombosis: A case report
 Petrous apex epidermoid cyst: A rare case
Petrous apex epidermoid cyst: A rare case
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


