KEY FACTS
Terminology
- •
Disorders of sexual development (DSD)
- •
Most common DSD if karyotype is XY (male)
- ○
Hypospadias: Urethra opens on underside of penis
- ○
Epispadias (less common): Urethra opens on top of penis
- ○
Cryptorchidism: Empty, small scrotum
- –
Often with small or abnormal penis
- –
- ○
- •
Most common DSD if karyotype is XX (female)
- ○
Clitoromegaly ± congenital adrenal hyperplasia (CAH)
- –
CAH causes virilization
- –
- ○
Prominent or fused labia (less common)
- ○
Imaging
- •
Hypospadias
- ○
Penis ends bluntly instead of normal taper
- –
Lateral echogenic lines at tip = prepuce folds
- –
- ○
Penis may be small and curved upward (chordee)
- ○
Tulip sign: Small, curved penis between scrotal folds
- ○
- •
Epispadias: Small, bifid penis
- ○
Associated with bladder extrophy
- ○
- •
Clitoromegaly (mimics small penis)
- ○
Associated prominent or fused labia mimic scrotum
- ○
CAD association: Adrenal glands may be large or normal
- ○
Clinical Issues
- •
Sex of fetus from genetic testing is key to diagnosis
- •
Some aspect of DSD seen in 1-2% of all live births
- •
Hypospadias in 1:200-250 males
- •
CAH is autosomal recessive (25% recurrence risk)
- •
Aneuploidy association: Trisomy 13, triploidy, trisomy 18
- •
Associated anomalies in 1/2 (most upper urinary tract)
Scanning Tips
- •
Do not assign sex at time of scan when DSD is suspected
- •
Pay attention to morphology of tip of phallus
- •
Look for testes in scrotum after 25 weeks
- ○
97% descended by 32 weeks
- ○
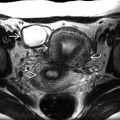
 tucked between small scrotum
tucked between small scrotum  without testes. The karyotype information is key to the diagnosis.
without testes. The karyotype information is key to the diagnosis.