KEY FACTS
Terminology
- •
Lethal skeletal dysplasia with 3 clinical subtypes
- ○
Type IA (poorly ossified skull, unossified spine)
- ○
Type IB (poorly ossified skull, rib fractures)
- ○
Type II (normal skull ossification)
- ○
Imaging
- •
Severe micromelia
- ○
All long bones are several standard deviations below mean for gestational age
- ○
- •
Disproportionately large head
- ○
Normal or deficient ossification depending on type
- ○
- •
Abnormal facies
- ○
Micrognathia, hypoplastic midface
- ○
- •
Lack of vertebral ossification is hallmark finding
- •
Short trunk with protuberant abdomen
- •
Short flared ribs, ± rib fractures depending upon type
- •
Polyhydramnios
- •
Hydrops in 1/3 of cases
Scanning Tips
- •
1st-trimester endovaginal ultrasound in high-risk patient (autosomal recessive inheritance in some types)
- ○
Cystic hygroma; increased nuchal translucency common in 1st trimester
- ○
Can be diagnosed as early as 12-14 weeks based on limb appearances
- ○
- •
In any fetus with visually shortened long bones
- ○
Measure femur:foot ratio ; if < 1, suggests skeletal dysplasia
- ○
Then, measure all long bones and compare to expected length for gestational age
- ○
- •
Other useful ratios in determination of lethal skeletal dysplasia
- ○
Femur length:abdominal circumference ratio < 0.16 suggests lethality
- ○
Chest circumference:abdominal circumference ratio < 0.8 suggests lethality
- ○
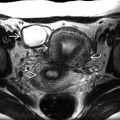
 , very small chest size
, very small chest size  , protuberant abdomen
, protuberant abdomen  , and complete lack of vertebral ossification
, and complete lack of vertebral ossification  . These are typical findings of achondrogenesis with the lack of vetebral ossification being the most specific. Carefully evaluate the spine in all skeletal dysplasia cases.
. These are typical findings of achondrogenesis with the lack of vetebral ossification being the most specific. Carefully evaluate the spine in all skeletal dysplasia cases.
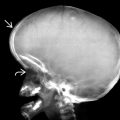
 . Note the prominent cheeks
. Note the prominent cheeks  and long philtrum
and long philtrum  .
.