Abstract
Uterine perforation and migration of intrauterine devices (IUDs) are rare complications that can present significant clinical challenges. We report the case of a 28-year-old woman who came in with a missed abortion at 11 weeks of gestation and was unexpectedly found to have an IUD embedded in the wall of her urinary bladder. She had a history of 5 pregnancies and a copper IUD was inserted a year ago. Although she presented with mild vaginal bleeding, there were no typical urinary symptoms to suggest a problem. However, imaging revealed the copper IUD had migrated outside the uterus and lodged in the bladder. After managing her pregnancy complications with evacuation and curettage, plans were made for surgical removal of the IUD. This case highlights how important it is to consider IUD migration, even when urinary symptoms are not present, in patients with unexplained pelvic issues. Early detection through imaging and prompt removal of the device are essential to prevent further complications. It also emphasizes the value of regular follow-up and patient education to ensure timely identification of potential issues before they escalate.
Introduction
Intrauterine devices (IUDs) are a common form of reversible contraception, widely acceptable due to their efficacy and relative safety [ ]. While they are mostly well-tolerated, pain and irregular bleeding are among the most common side effects, particularly during the initial months of their use. Some serious complications associated with IUD use can include pelvic inflammatory disease, contraceptive failure, expulsion, uterine perforation, or migration of the device to adjacent organs [ ].
Uterine perforation is considered one of the most serious complications related to the use of IUD. The frequency of this complication is estimated to be between 0.05 and 13 per 1000 insertions (average, 1.2/1000) with subsequent migration from the uterine cavity into adjacent organs such as omentum, the broad ligament, pouch of Douglas, colon, mesentery, urinary bladder, and sigmoid [ ]. Approximately, 2% of migrated IUDs may involve the bladder [ , ].
The clinical presentation of IUD embedded in the urinary bladder varies but mostly includes lower urinary tract symptoms such as frequency, urgency, dysuria, and hematuria. Less commonly, patients may also experience dyspareunia or other forms of sexual dysfunction [ ].
Early recognition and treatment are essential to prevent further complications and alleviate symptoms, so it’s recommended that when the IUD strings are not detected during examination, transvaginal ultrasound or other imaging studies such as CT or MRI should be conducted before concluding that the device has been expelled [ ].
Management of an intravesical IUD typically involves surgical removal, which can be achieved through endoscopic procedures or, in more complex cases, open surgery. Additionally, regular follow-up and patient education on the importance of monitoring IUD position can help in early detection of such complications [ ].
Case presentation
A 28-year-old pregnant patient, gravida 5, para 4, at 11 weeks of gestation, was referred to the hospital as a case of incomplete abortion. She presented with mild vaginal bleeding, without associated abdominal pain, palpitations, or other complaints. Due to this presentation, she was initially diagnosed as a case of missed abortion and started on a cytotoxic medication, 2 tablets every 4 hours. Her current pregnancy had been uneventful until the onset of these symptoms. Notably, all her previous pregnancies resulted in uncomplicated vaginal deliveries. She reported a history of intrauterine device (IUD) insertion 1 year ago. The patient denied any history of chronic illnesses or previous surgeries. Her family history was unremarkable, and she was not on any chronic medications. Additionally, she reported no known allergies. She is a nonsmoker and does not consume alcohol.
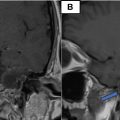
On initial examination, the patient was conscious, alert, and oriented. Her vital signs were stable, with a blood pressure of 111/70 mmHg, a pulse of 77 beats per minute, and an oxygen saturation of 99% on room air. A bimanual vaginal examination revealed mild vaginal bleeding. Ultrasonography showed retained products of conception measuring approximately 1.7 mm and abdominal and pelvic computed tomography (CT) scan showed a copper intrauterine device (IUD) displaced outside the uterus, in the urinary bladder wall, as shown in Figs. 1 and 2 . The specialist was informed, and the patient was admitted. Intravenous access was established, and intravenous fluids were initiated at a rate of 3 liters per 24 hours. Comprehensive laboratory tests were ordered, including serial complete blood counts (CBC) every 6 hours, along with a serial collection of pads for bleeding assessment.

Related posts:
 Breast cancer with medullary features shows a fast and plateau enhancement pattern on magnetic resonance images: A case report
Breast cancer with medullary features shows a fast and plateau enhancement pattern on magnetic resonance images: A case report
 A rare and life-threatening case of spontaneous hemopneumothorax presenting with severe hemodynamic instability
A rare and life-threatening case of spontaneous hemopneumothorax presenting with severe hemodynamic instability
 Avascular necrosis of lateral femoral condyle in a middle-aged woman from central India
Avascular necrosis of lateral femoral condyle in a middle-aged woman from central India
 A very rare case of ileocolic and appendiceal intussusception with acute appendicitis
A very rare case of ileocolic and appendiceal intussusception with acute appendicitis
 Rare case of left epididymo-orchitis complicated by pampiniform plexus thrombosis: A case report
Rare case of left epididymo-orchitis complicated by pampiniform plexus thrombosis: A case report
 Petrous apex epidermoid cyst: A rare case
Petrous apex epidermoid cyst: A rare case
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


