KEY FACTS
Imaging
- •
Ill-defined, hypoechoic tumor diffusely involving entire lobe or gland, often invading adjacent structures
- •
Background of multinodular goiter or differentiated thyroid cancer
- •
Typically > 5 cm at presentation
- •
Necrosis (78%), dense amorphous calcification (58%)
- •
Extracapsular spread with infiltration of trachea, esophagus, & perithyroid soft tissues & nerves
- •
May see thrombus in internal jugular vein & carotid artery, causing expansion & occlusion of vessels
- •
Color Doppler shows prominent, small, chaotic intratumoral vessels
- •
Nodal or distant metastases in 80% of patients
- ○
Abnormal vascularity seen within metastatic nodes
- ○
Top Differential Diagnoses
- •
Differentiated thyroid carcinoma
- •
Non-Hodgkin lymphoma
- •
Thyroid metastases
Clinical Issues
- •
Rapidly growing, large, painful neck mass, 1-2% of thyroid malignancy
- •
Presents at later age than other thyroid malignancies, most typically 6th or 7th decade
- •
50% have associated symptoms from local invasion: Dyspnea, hoarseness, or dysphagia
- •
Rapidly fatal, mean survival of 6 months after diagnosis
Scanning Tips
- •
Rapidly enlarging, infiltrative thyroid mass suggests anaplastic carcinoma or thyroid non-Hodgkin lymphoma; biopsy essential for diagnosis
- •
Use curvilinear transducer to encompass entire tumor when large
- •
Ultrasound may be unable to completely evaluate infiltration into trachea, larynx, adjacent soft tissues, & mediastinal spread; CECT or MR may be necessary
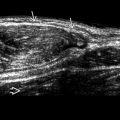
 [T4a (stage IVa) disease].
[T4a (stage IVa) disease].
 and extending anterolaterally
and extending anterolaterally  . There is invasion of the sternocleidomastoid muscle
. There is invasion of the sternocleidomastoid muscle  and compression of the internal jugular vein
and compression of the internal jugular vein  . The common carotid artery was normal
. The common carotid artery was normal  .
.
 . The mass is heterogeneous in echotexture.
. The mass is heterogeneous in echotexture.