Cerebral Metastases
Shaun R. Wagner
CLINICAL HISTORY
57-year-old female with new onset of focal seizures. Medical history positive for breast cancer diagnosed and treated 3 years ago.
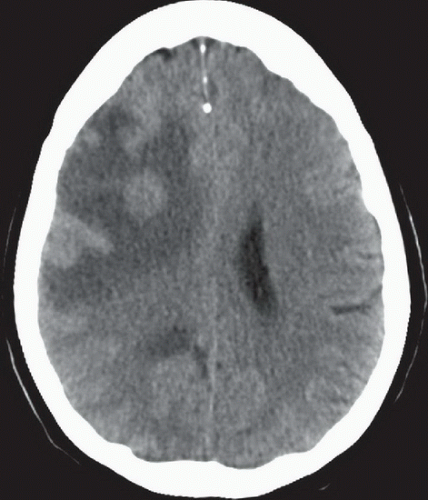 FIGURE 13A |
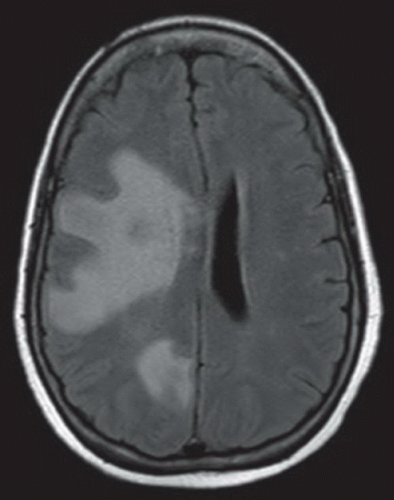 FIGURE 13B |
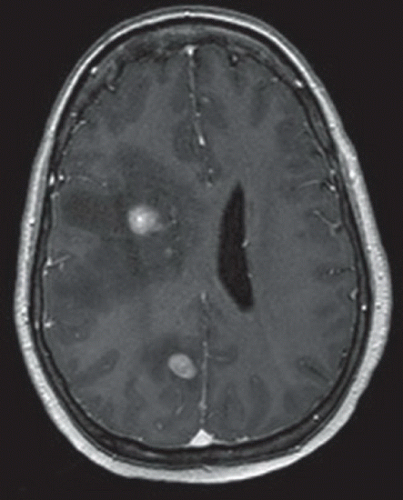 FIGURE 13C |
FINDINGS
Figure 13A: Axial noncontrast CT image through the brain at the level of the lateral ventricles demonstrates a mass that is isodense to gray matter within the right frontal corona radiata white matter with marked surrounding vasogenic edema. A second subtle area of vasogenic edema is seen posteriorly along the medial right occipital lobe. Figure 13B: Axial FLAIR image at approximately the same level as the CT demonstrates extensive hyperintense signal within the subcortical white matter of the right frontal and occipital lobes consistent with vasogenic edema. Figure 13C: Axial postcontrast T1 image demonstrates enhancement of the mass seen on CT as well as another enhancing lesions that was not delineated on CT imaging.
DIFFERENTIAL DIAGNOSIS
There is a short list of common differentials for multifocal lesions in the brain. Primary among these considerations are metastases and multifocal abscesses. Multifocal metastases demonstrate enhancement on postcontrast CT and MRI in variable patterns from solid to nodular or peripheral and ringlike, while abscesses generally demonstrate a thin peripheral rim of enhancement. Additionally, pyogenic abscesses classically show central hyperintensity on diffusion-weighted imaging (DWI) and low signal intensity reflecting restricted diffusion on apparent diffusion coefficient (ADC) maps. Ring-enhancing
metastases generally demonstrate facilitated diffusion (bright on DWI and ADC) centrally in the nonenhancing portions of the lesion. T2 imaging will also characteristically demonstrate hypointensity within an abscess capsule. Multiple sclerosis (MS) may also present with multiple, possibly incomplete, ring-enhancing parenchymal lesions corresponding to active demyelination plaques. Rarely, MS plaques can reach substantial size and exert mass effect in the tumefactive variant. MS lesions generally demonstrate T2 hyperintensity and are oriented perpendicular to the ventricles. Involvement of the corpus callosum is common in MS, whereas callosal involvement is distinctly uncommon in most other differentials, except this last differential diagnosis. Glioblastoma may present as multiple enhancing lesions within the brain. Necrosis and hemorrhage are very common in glioblastoma.
metastases generally demonstrate facilitated diffusion (bright on DWI and ADC) centrally in the nonenhancing portions of the lesion. T2 imaging will also characteristically demonstrate hypointensity within an abscess capsule. Multiple sclerosis (MS) may also present with multiple, possibly incomplete, ring-enhancing parenchymal lesions corresponding to active demyelination plaques. Rarely, MS plaques can reach substantial size and exert mass effect in the tumefactive variant. MS lesions generally demonstrate T2 hyperintensity and are oriented perpendicular to the ventricles. Involvement of the corpus callosum is common in MS, whereas callosal involvement is distinctly uncommon in most other differentials, except this last differential diagnosis. Glioblastoma may present as multiple enhancing lesions within the brain. Necrosis and hemorrhage are very common in glioblastoma.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


