Abstract
Parathyroid ultrasound is widely used in clinical practice and plays a crucial role in the diagnosis and treatment of parathyroid diseases. Nevertheless, ultrasound physicians frequently encounter a number of challenges and doubts in their professional practice. For this reason, Superficial Organs and Peripheral Vessels Committee of Chinese Association of Ultrasound in Medicine and Engineering has formulated the expert consensus on certain common clinical problems of parathyroid ultrasound based on the current research progress and clinical experience, in order to guide the clinical practice. This consensus describes in detail the diagnostic and interventional common problems of parathyroid ultrasound and provides in-depth discussion on related contents.
Introduction
The parathyroid gland is a vital endocrine gland in the human body. The parathyroid hormone (PTH) it secretes can act directly or indirectly on tissues and organs, including bones, kidneys and the small intestine, in order to regulate and maintain blood calcium levels. A substantial body of evidence from previous studies has demonstrated a correlation between a number of diseases and the parathyroid gland. Therefore, the diagnostic and treatment procedures are of paramount importance in the management of the parathyroid gland. In the past two decades, ultrasound has been widely used in the diagnosis, preoperative localization, and intraoperative guidance of parathyroid diseases. However, the appropriate application of ultrasound in the management of thyroid diseases continues to present a number of challenges. To meet the need for a detailed focus on parathyroid ultrasound, the Chinese Association of Ultrasound in Medicine and Engineering, Subgroup on Superficial Organs and Peripheral Vessels developed an expert consensus on the most prevalent clinical issues associated with parathyroid ultrasound based on a systematic literature review and clinical experience.
Methods
The expert panel consists of radiologists from various provinces and cities in China, all of whom are renowned experts in their fields and have long been engaged in research on parathyroid diseases. During 2023, the panelists sent out questionnaires across the country via the internet to find out what issues related to parathyroid ultrasound were of most concern in their work. 2939 questionnaires were answered. Nineteen problems related to the diagnosis and interventional treatment of parathyroid disease were identified. After that, the panel conducted a systematic literature search using the National Library of Medicine based on the topics and keywords of these 19 questions. Combined with the results of the literature review and clinical experience, the panel discussed and reviewed these 19 questions and reached consensus recommendations.
The consensus recommendation is written with reference to the grading system of evidence-based guidelines and is applied to two parts: the class of recommendation and the level of evidence. Recommended levels: Level I refers to procedures or treatments that have been proven and consistently accepted to be beneficial, useful and effective; Level II refers to procedures or treatments for which the evidence of usefulness or effectiveness is conflicting or there are differing views (Level IIa means that the evidence/opinion tends to be useful and effective and the use of these procedures or treatments is reasonable; Level IIb means that the evidence/opinions are not sufficiently proven to be useful and could be considered for use); Level III refers to procedures or treatments that have been proven and consistently recognized to be useless and ineffective, and in some cases may be harmful, and are not recommended. Evidence levels: Level A refers to data from multiple randomized clinical trials or meta-analyses; Level B refers to data from a single randomized clinical trial or multiple nonrandomized controlled trials; Level C refers to data derived from expert consensus opinion or small clinical trials or retrospective studies.
Although this consensus has been critically reviewed by the panel, it cannot be used as the sole criterion for the management of parathyroid disease and may need to be individually adjusted by physicians in a clinical setting. In addition, this Consensus Statement is intended solely as a reference tool for medical personnel in the industry and does not have the force or effect of law.
Diagnostic part
Q1: What is the echogenicity and morphology of the normal parathyroid glands? What are the abnormal sonographic manifestations?
Expert opinion
81.79% of people were able to detect at least one normal parathyroid gland through US, with the inferior parathyroid glands being significantly more detectable by US compared to the superior ones. Among the normal parathyroid glands detectable by US, 19.85% are the superior parathyroid glands and 80.15% are the inferior parathyroid glands [ , ]. In individuals undergoing surgery for primary hyperparathyroidism, ectopic parathyroid glands are found in approximately 6% to 16% of cases [ ]. For inferior parathyroid glands, the anterior mediastinum (particularly within the thymus gland) represents the most common ectopic location, with intrathymic localization accounting for approximately 30% of cases. Other documented but less frequent inferior gland locations include the anterosuperior mediastinum (22%), intrathyroidal space (15%–22%), and rarely the submandibular region (9%). Superior parathyroid glands demonstrate distinct ectopic distribution patterns, most frequently appearing in the tracheoesophageal groove (43%), followed by retroesophageal (22%), posterosuperior mediastinal (14%), intrathyroidal (7%), and carotid sheath (7%) locations [ ]. Before puberty, the parathyroid glands primarily consist of chief cells. At the onset of puberty, fat particles begin to appear within these chief cells. At the same time, adipose tissue starts to form between the chief cells and progressively increases with age until around 40 years old, after which the fat content in the gland remains relatively stable. Therefore, normal parathyroid glands after the onset of puberty commonly appear as homogeneous hyperechoic texture (79.29%) with the regular shape (97.5%), and hyperechoic capsule visible on some of the periphery (97.21%) on ultrasound (US) [ ]. If some or all of the parathyroid glands exhibit hypoechoic or nonechoic texture after puberty, which should be regarded as abnormality [ ].
The superior parathyroid glands and the thyroid originate from the fourth pharyngeal pouch. The position of the parathyroid glands is relatively constant, most of which are located at the junction of the middle and upper one-third of the posterior aspect of the lateral lobe of the thyroid and nearby areas. The parathyroid glands possess greater spatial allowance at their cephalic side and the foot side, thus commonly exhibiting an elliptical shape in long-axis sections. However, owing to their close proximity to structures such as the trachea, thyroid, and longus colli on both lateral and anteroposterior sides, which results in limited space, their short-axis sections may present irregular shapes, including triangular, crescent-like, and various other casting growth patterns.
The inferior parathyroid glands, along with the thymus, originate from the third pharyngeal pouch. During development, they migrate to the foot side in the shallow direction of the superior parathyroid glands, and their positions change greatly. However, most are located near the lower pole of the thyroid and within the fatty thymus, where they are generally not compressed by surrounding solid organs. Consequently, both their long-axis and short-axis sections typically exhibit elliptical or circular shapes [ ]. Nonetheless, a portion of the inferior parathyroid glands may be positioned between the thyroid and the carotid artery, leading to irregular shapes with casting growth patterns in their short-axis sections.
Expert recommendation 1: The normal parathyroid glands commonly appear as homogeneous hyperechoic on US after puberty. If some or all of the parathyroid glands exhibit hypoechoic or nonechoic features after puberty, this should be regarded as abnormality. Recommendation level: I; Evidence level: B.
Q2: How to conduct standardized protocol for the US examination and image acquisition of parathyroid glands?
Expert opinion
The frequency of the probe for parathyroid US is commonly 7.5–12.0MHz, and a higher frequency probe can be used to improve the image resolution. When the parathyroid glands are not detectable at the normal position, a lower frequency band probe can be selected to scan behind the clavicle or sternum to search for any ectopic parathyroid glands.
The patient is positioned with a pillow placed beneath the shoulders, facilitating a posterior neck extension and hyperextension. The scanning scope should encompass transverse sections extending from the carotid bifurcation to the thoracic inlet, as well as longitudinal sections from the carotid artery to the ipsilateral paratracheal region, with taking the lateral lobe of the thyroid as the central landmark into account. Owing to the possibility that parathyroid glands may be hidden in the lower neck, upper mediastinum, or beneath the clavicle, instructing patients to swallow during examination and conducting real-time observation can significantly assist in the detection of ectopic lesions. Furthermore, color and/or power Doppler US typically demonstrates color flow signals in normal parathyroid glands or parathyroid lesions [ ].
Attention should be paid to the acquisition of images, when abnormalities in the parathyroid glands are found. The imaging process should encompass both transverse and longitudinal sections. In the transverse section, efforts should be made to delineate the relationship of the lesion with the thyroid, trachea, esophagus, and common carotid artery. The longitudinal section should aim to illustrate the association of the lesion with the upper or lower pole of the thyroid as far as possible. The location, number, and size of the abnormal parathyroid glands should be recorded. For size measurement, three dimensions should be recorded. Additionally, a detailed description of the relationship between the abnormal parathyroid glands and the adjacent structures, including the thyroid, trachea, esophagus, and common carotid artery, should be described [ , ].
Expert recommendation 2: Standardized examination and image storage of the parathyroid glands can reduce misdiagnosis and missed diagnoses of parathyroid disease. Recommendation level: I;Evidence level: B.
Q3: Is it necessary to measure the size of each parathyroid glands during US examination? What is the significance of the size of the parathyroid glands?
Expert opinion
Normal parathyroid glands are typically not all easily visualized, with the inferior parathyroid glands exhibiting a higher display rate. It is common for each parathyroid gland to have a volume below 40 mm³ (0.04 cm³) [ ]. Normal parathyroid glands commonly appear as hyperechoic texture, and there is not necessary to measure the size of each parathyroid glands [ ]. However, when parathyroid diseases occur, due to a reduction or absence of fat content within the tissue, they often show hypoechoic. In such instances, measuring the size of the lesions becomes necessary.
The significance of the size of the parathyroid glands in US examination includes the following aspects:
- 1.
Monitoring disease progression: Changes in the size of the parathyroid glands serve as a crucial indicator for assessing disease progression. Previous studies have demonstrated a positive correlation between the size of the parathyroid glands and serum parathyroid hormone (PTH) levels in patients with hyperparathyroidism (HPT), suggesting that measurements of parathyroid glands size can predict PTH levels. In hemodialysis patients, the size of the parathyroid glands is associated with PTH levels, hemodialysis duration, and the effects of drug treatment, thus aiding in the monitoring of related endocrine conditions and treatment efficacy. If an increase in the size of the parathyroid glands is observed during follow-up, this indicates that the disease may be progressing and that further diagnosis and intervention is needed.
- 2.
Differential diagnosis: The variation in the size of the parathyroid glands can, to some extent, assist in differentiating the nature of the lesion. A stable-sized parathyroid gland is more likely to indicate a benign lesion [ ].
- 3.
Determining follow-up frequency: Changes in the size of the parathyroid glands can assist in deciding the frequency of follow-up. Patients with significant changes in gland volume may require more frequent follow-ups to promptly detect any alterations in their condition and implement appropriate interventions.
Expert recommendation 3: The size of the parathyroid glands holds significant importance in follow-up observations conducted via US. Monitoring changes in their size through US can effectively assess disease progression and guide clinical decision-making. Recommendation level: IIa;Evidence level: C.
Q4: If the parathyroid glands are visualized on US in patients with no relevant clinical symptoms, is it necessary to described this sonographic finding in the report? How to indicate in this situation?
Expert opinion
Since normal parathyroid glands are commonly hyperechoic on US, it is usually not necessary to indicate when patients have no relevant clinical symptoms. However, for parathyroid glands with potential pathological risk that require further monitoring or assessment, an indication is warranted to ensure comprehensive clinical data recording and subsequent diagnostic and therapeutic measures. When the parathyroid glands appear hypoechoic on US, it is essential to include an indication in the report. The following are recommendations for making such indications in the report.
- 1.
Description of the sonographic features of the parathyroid glands [ ]:
- a.
Location: The relative position of the parathyroid glands to surrounding anatomical structures (such as the thyroid, trachea, and carotid artery), including the distance of nodules from the surface or edge of the lateral lobes of thyroid.
- b.
Size (for those requiring further monitoring and assessment of potential disease risks): Record the three diameters of the parathyroid glands.
- c.
Morphology: Describe the morphological characteristics of the parathyroid glands (e.g., whether the shape is regular, whether the margin is circumscribed).
- d.
Echogenicity: Describe the echogenicity of the parathyroid glands, such as hypoechoic, isoechoic, or hyperechoic.
- e.
Vascularity: Describe the vascularity using color Doppler flow imaging.
- a.
- 2.
Recommendation: If necessary, consider regular follow-up to monitor changes in the parathyroid glands [ ].
Expert recommendation 4: When the parathyroid glands are detected on US in patients with no relevant clinical symptoms, only the lesions with suspicious sonographic features should be recorded and described. Recommendation level: IIa; Evidence level: C.
Q5: When multiple abnormal parathyroid glands are detected on US, how to standardized describe their location? Describe only the big ones or record them individually?
Expert opinion
When multiple abnormal parathyroid glands are detected on US, it is necessary to document each abnormal gland individually, providing detailed descriptions of their locations, sizes, morphologies, and echogenic characteristics. This method ensures comprehensive diagnostic information, facilitating subsequent clinical management and treatment.
In the US report, the abnormal nodule with the largest volume should be described first, followed by a sequential account of any additional abnormal nodules identified. For guidance on specific description method, refer to Question 4 [ ].
Additionally, schematic diagrams can be utilized to clearly mark the location and size of each abnormal nodule. This visual representation assists clinicians in quickly identifying and comprehending the exact locations of these nodules when reviewing the US report [ ].
Expert recommendation 5: Standardized recording and description of each parathyroid gland with suspicious sonographic features facilitates the formulation of subsequent diagnosis and treatment. Recommendation level: I; Evidence level: B.
Q6: In addition to differences in clinical symptoms, how to distinguish parathyroid hyperplasia from parathyroid adenoma through US? When US is unable to differentiate between these two diseases, is the final treatment procedure affected?
Expert opinion
Parathyroid adenomas are the predominant etiology of primary hyperparathyroidism (PHPT), responsible for approximately 80% to 85% of cases, whereas parathyroid hyperplasia accounts for about 15% of PHPT instances [ ]. Both parathyroid hyperplasia and parathyroid adenoma exhibit as hypoechoic nodules (96.8%) with rich vascularity on US (77.7%), rendering differentiation between the two challenging [ , , ]. However, the majority of parathyroid adenomas manifest as solitary nodules. Multiple parathyroid adenomas (more than one nodule) are uncommon in standard PHPT cases, with a prevalence of between 2% to 5%. Conversely, parathyroid hyperplasia can involve multiple glands more than 90% of the time [ ] and is predominantly seen in patients with multiple endocrine neoplasia (MEN) or as a secondary condition in those with renal disease (especially postdialysis), vitamin D deficiency or malabsorption, and specific medication therapies. Therefore, when multiple parathyroid lesions are detected by US, parathyroid hyperplasia should be the primary consideration, and all four parathyroid glands should be individually evaluated to avoid omissions.
The differentiation between parathyroid adenoma and parathyroid hyperplasia holds significant importance primarily for patients scheduled for surgery. This is because in patients with parathyroid hyperplasia, the degree of hyperplasia often varies among individual parathyroid glands, and overlooking smaller hyperplastic parathyroid glands can lead to suboptimal surgical treatment [ ]. Consequently, when assessing US findings in these patients prior to surgery, it is essential to take into account the patient’s clinical history, including chronic kidney disease or genetic syndromes like MEN1, which may suggest hyperplasia [ ]. Biochemical markers such as increased parathyroid hormone and calcium levels contribute to the diagnostic process [ ]. Imaging techniques, including 99mTc-Sestamibi scans, 4D-CT, and MRI, are essential for the identification of ectopic glands and the differentiation between mono-glandular and polyglandular diseases [ ].
Expert recommendation 6: Parathyroid hyperplasia and parathyroid adenoma are difficult to be accurately distinguished from conventional US features, and the number of involved glands has a certain auxiliary value in the differential diagnosis between the two conditions. Recommendation level: IIb;Evidence level: C.
Q7: How to make differential diagnosis of parathyroid glands, Zuckerkandl’s tubercle (ZT), dorsal space occupying lesion of thyroid, and central neck lymph node?
Expert opinion
Zuckerkandl’s tubercle (ZT) represents a protrusion of normal thyroid tissue extending from the posterior or posteromedial margin of the thyroid into the tracheoesophageal groove. The pooled prevalence estimate of a ZT was 70.2% in the general population [ ]. ZT can overlap with the lateral lobe of the thyroid when the size relatively large. Given that ZT is encapsulated by two layers of thyroid capsule, it is prone to be erroneously identified as an abnormal nodule in the lateral lobe of the thyroid on US. However, the echogenicity of ZT is identical to that of the thyroid, and it is distinctly separated from the thyroid by an anterior capsule, often exerting no compression on the thyroid. When scanned from multiple planes and angles, the pedicle of ZT connecting to the thyroid becomes visible, whereas the parathyroid glands remain unconnected. Careful observation of the adjacency relationship between the lesion and the thyroid is crucial for differentiating parathyroid disease from ZT [ ].
Space-occupying lesions located on the dorsal side of the thyroid, due to their origin from thyroid tissue, typically lack a strong echogenic capsule separating them from the thyroid. The blood supply of these lesions originates from the nearby thyroid tissue, without an independent feeding artery, which contrasts with the majority of parathyroid glands that possess distinct parathyroid arteries for their blood supply. These features are instrumental in differentiating space-occupying lesions located on the dorsal side of the thyroid from parathyroid lesions.
Central neck lymph nodes are typically hypoechoic, posing a certain degree of challenge in differentiating them from parathyroid lesions by US. When enhancing the gain of gray-scale US, a linear high-echoic hilar structure can be observed within some lymph nodes, and the internal vascularity of these lymph nodes in the central neck region is generally scarce or difficult to discern. Conversely, parathyroid glands do not possess such a high-echoic hilar structure, and the majority of abnormal parathyroid glands show abundant blood signal (77.7%) [ ]. These distinct sonographic features facilitate the differentiation of abnormal parathyroid glands from central neck lymph nodes [ ].
Expert recommendation 7: The internal echogenicity, color Doppler flow signal, and adjacent relationship with the surrounding tissue are helpful in the differential diagnosis of the parathyroid gland, ZT, dorsal space occupying lesion of the thyroid, and central neck lymph nodes. Recommendation level: IIa; Evidence level: C.
Q8: Should dialysis patients undergo routine US examinations of the parathyroid glands? What are matters needing attention?
Expert opinion
Routine parathyroid US examination holds significant importance for dialysis patients. These patients often exhibit mineral metabolism disorders, leading to the development of secondary hyperparathyroidism (SHPT). Ultrasonography can detect parathyroid abnormalities at an early stage, such as parathyroid hyperplasia or nodule, so as to facilitate early treatment and intervention, such as drug therapy, parathyroidectomy or ablation, and avoid the occurrence of serious complications [ ].
Notes for US examination:
- 1.
Examination frequency: For patients undergoing long-term dialysis, it is recommended to conduct a parathyroid US examination every 6–12 months. The specific frequency can be adjusted based on the patient’s condition, laboratory results, and clinical symptoms.
- 2.
US equipment and sonographers: High-resolution US equipment should be utilized, equipped with experienced sonographers to ensure the accuracy and reliability of the examination. Sonographers should be proficient in the anatomical characteristics and pathological changes of the parathyroid glands.
- 3.
Laboratory examination: The US examination should be integrated with the patient’s serum calcium, phosphorus, PTH levels, and 25-hydroxyvitamin D levels for a comprehensive evaluation, thereby avoiding the pitfalls of basing diagnostic judgments solely on a single indicator.
- 4.
Multidisciplinary treatment: For the parathyroid abnormalities detected through US examination, it is crucial to maintain close collaboration with departments such as endocrinology, nephrology, and other imaging departments to formulate therapeutic regime and follow-up strategies for patients.
Expert recommendation 8: Regular parathyroid US examination combined with laboratory examination is of great significance for the management of long-term dialysis patients. Recommendation level: IIa;Evidence level: B.
Q9: When multiple endocrine neoplasia (MEN) syndromes are clinically suspected, what is the recommended approach for evaluating the parathyroid glands using US? Furthermore, which additional organs should undergo US evaluation in these cases?
Expert opinion
MEN syndromes are rare autosomal dominant hereditary disorders characterized by the simultaneous or sequential development of two or more endocrine tumors in patients. MEN syndromes can be categorized into four types: MEN1, MEN2A, MEN2B, and MEN4 [ , ].
MEN1 is a rare (prevalence 3-20/100000) highly penetrant autosomal dominant disorder [ ]. The characteristic manifestation of MEN1 syndrome is PHPT, with multiple hyperplastic and neoplastic changes in the parathyroid glands, but it can be asymmetrical and asynchronous. Other tumors significantly associated with MEN1 include pituitary adenomas/pituitary neuroendocrine tumors (NETs), duodenal-pancreatic NETs, as well as NETs of the gastrointestinal tract, lungs, and thymus, and adrenal cortical tumors. Consequently, we should pay particular attention to the assessment of the pancreas, adrenal glands, and gastrointestinal tract in such patients via US examination [ ].
MEN2A, comprising 90%–95% of MEN2, may also be accompanied by parathyroid hyperplasia or parathyroid adenoma. MEN2A often manifests as mild enlargement of a single or multiple parathyroid glands, yet symptoms of HPT are typically mild. The characteristic manifestations of MEN2 syndrome are medullary thyroid carcinoma (MTC) and phaeochromocytoma [ ]. Therefore, we should pay more attention to the assessment of the thyroid and adrenal glands via US.
Expert recommendation 9: Patients with HPT accompanied by multiple glandular abnormalities should undergo genetic counseling and undergo detailed screening of potentially affected tissues and organs, such as the thyroid and adrenal glands. Recommendation level: I;Evidence level: A.
Q10: What is the clinical application value of contrast-enhanced ultrasound (CEUS) in the diagnosis of parathyroid disease?
Expert opinion
CEUS can provide a real-time, dynamic, and quantitative evaluation of blood perfusion in parathyroid tissues or lesions. This technique exhibits certain advantages in the identification of parathyroid lesions, preoperative localization, and postablation assessment [ ].
- 1.
CEUS facilitates the differentiation of parathyroid lesions. CEUS can differentiate between parathyroid nodules, thyroid nodules, and lymph nodes by analyzing the enhancement and washout patterns of the lesions. In comparison to the thyroid tissue, normal parathyroid glands during CEUS typically exhibit simultaneous enhancement and iso-enhancement, whereas parathyroid lesions predominantly manifest as rapid and hyperenhancement. Previous studies have demonstrated that parathyroid hyperplasia is characterized by diffuse and homogeneous enhancement and wash-out appearance, whereas parathyroid adenomas show centripetal enhancement with prominent rim enhancement, accompanied by visible polar feeding vessels at the periphery.
- 2.
CEUS facilitates the preoperative localization of microwave ablation (MWA) for PHPT. Especially for multiple parathyroid lesions, the sensitivity of CEUS (100%) for localization is significantly higher than that of conventional US (75%) and 99mTc-MIBI (65.62%) ( p < 0.05) [ ].
- 3.
CEUS can be utilized to evaluate the post-MWA ablation status of parathyroid disease. The complete ablation is indicated if no enhancement is observed in the lesion area. Conversely, the presence of a peripheral ring-like or local enhancement zone around the ablation area indicates incomplete ablation, necessitating additional ablation procedures. CEUS immediately after ablation may interfere with image quality due to temporary occlusion of capillaries or tissue carbonization, and reexamination 1–2 days after ablation can more accurately reflect the actual blood supply [ ].
Patients with parathyroid nodules who undergo ablation followed by CEUS examination are considered to have undergone complete ablation if no enhancement is observed in the lesion area. Conversely, the presence of a peripheral ring-like enhancement zone around the ablation area indicates incomplete ablation of the lesion, necessitating additional ablation procedures.
Expert recommendation 10: CEUS exhibits several advantages in the recognition, preoperative localization, and postablation evaluation of parathyroid lesions. Recommendation level: IIa; Evidence level: B.
Intervention part
Q11: When is a parathyroid biopsy necessary? How to choose the biopsy method?
Expert opinion
Indications for parathyroid biopsy: [ ] confirmation of suspected parathyroid lesions before surgery/ablation; [ ] differential diagnosis between parathyroid lesions and those originating from the thyroid, lymph nodes, and other tissues.
For PHPT, it is not recommended to perform fine-needle aspiration (FNA) biopsy before surgery except for a few special and complex PHPT cases. If parathyroid cancer is suspected, a biopsy should not be performed [ ]. Due to the risk of needle dissemination, FNA biopsy for suspected primary lesions are not recommended before the first surgery. When the nature of the metastatic lesion cannot be clearly defined by various imaging examinations, FNA biopsy on the tissue of the metastatic lesion can be considered as appropriate, because at this time, the metastatic lesion is already there, and the concern about needle dissemination caused by FNA biopsy is much smaller than that of the primary lesion [ ].
Fine-needle aspiration cytology (FNAC) is the preferred biopsy method. To confirm the diagnosis, immunocytochemical indicators of PTH can be added to the cell smears, or PTH detection in the washout fluids of FNA specimens can be used to diagnose lesions originating from the parathyroid [ ]. The measurement of PTH in the washout fluids is highly sensitive and requires only PTH or cellular fragments remaining on the inner wall of the puncture needle. The measurement of PTH in FNA washout fluids (US-FNA PTH) provides an effective preoperative localization method for patients with unclear preoperative imaging localization and recurrence of PHPT requiring reconfirmation of the lesion [ ]. The puncture needle must be changed when multiple target biopsies are taken.
Expert recommendation 11: Parathyroid biopsy is primarily used for preoperative confirmation of suspected lesions or differentiation of their origin, and is not routinely recommended for qualitative diagnosis of pathological classification. FNA combined with PTH detection is the preferred method to enhance accuracy. Recommendation level: IIa;Evidence level: B.
Q12: What is the value of PTH in FNA washout fluids in the diagnosis and differential diagnosis of parathyroid diseases?
Expert opinion
PTH is an alkaline single-chain polypeptide hormone secreted by the chief cells of the parathyroid gland. The increase of US-FNA PTH can suggest that the target lesion is of parathyroid origin. The clinical applications are as follows:
- 1.
When parathyroid lesions present as cystic masses, US-FNA PTH can aid in determining whether the cystic masses are of parathyroid origin. The PTH value of parathyroid cyst can be two times to several thousand times of the upper limit of normal PTH measurement in serum [ , ].
- 2.
US-FNA PTH is superior to other imaging modalities in improving the accuracy of preoperative detection of parathyroid adenomas, especially in patients with coexisting thyroid nodules [ ].
- 3.
For patients with previously diagnosed and treated parathyroid carcinoma, US-FNA PTH can be used to differentiate scar tissue from recurrent or metastatic disease [ ].
- 4.
Intraoperatively, US-FNA PTH facilitates rapid identification of parathyroid tissue to distinguish it from thyroid lesions or other tissues such as fat and lymph nodes, enhancing the accuracy of parathyroid localization. This is particularly important in patients with unsuccessful previous exploratory surgery but persistent hypercalcemia.
Parathyroid carcinoma is a rare disease accounting for less than 1% of PHPT. In cases of suspected parathyroid carcinoma, FNA is not recommended prior to initial surgery due to the technical difficulty in distinguishing benign from malignant disease on cytological specimens and the potential risk of tumor dissemination along the needle tract, possibly leading to recurrence. Additionally, there are some limitations in the application of US-FNA PTH, as the diagnostic criteria currently varies. Combining FNAC and immunohistochemical staining can further improve diagnostic accuracy.
Expert recommendation 12: Elevated PTH in FNA washout fluids suggests that the target lesion is of parathyroid origin. Recommendation level: I; Evidence level: B.
Q13: Can parathyroid disease be treated by thermal ablation? How to select indications?
Expert opinion
Traditional treatment methods for parathyroid diseases include drug therapy and surgical excision. However, thermal ablation techniques have gradually been applied to the treatment of parathyroid diseases in recent years. Thermal ablation can be used for HPT, including PHPT, SHPT, and tertiary hyperparathyroidism (THPT) [ ].
The selection of indications for thermal ablation requires careful assessment, encompassing factors such as the patient’s age, health status, comorbidities, severity of symptoms, as well as the size and location of the lesion. The currently recognized indications primarily include:
- 1.
Patients with symptomatic PHPT.
- 2.
Asymptomatic PHPT patients with one of the following conditions: (a) serum calcium levels above the normal range, (b) significantly decreased bone mineral density with a higher likelihood of fragility fractures, (c) creatinine clearance < 60 mL/min.
- 3.
Thermal ablation for PHPT may be considered for older patients or those with severe comorbidities who are deemed unsuitable for surgical intervention.
- 4.
Thermal ablation therapy can be considered for PHPT during pregnancy, because thermal ablation does not require general anesthesia. Regardless of gestational age, thermal ablation is a more suitable alternative to parathyroidectomy [ ].
- 5.
Patients with SHPT who have failed drug therapy.
- 6.
For certain patients, such as those with recurrent HPT after parathyroidectomy, who may be deemed unsuitable for repeat surgery due to scarring, adhesions, and tissue destruction, US-guided ablation therapy is recommended as an alternative due to its precision and minimally invasive nature [ , ].
The contraindications include:
- 1.
Suspected parathyroid carcinoma: A thorough assessment of clinical symptoms, laboratory results, suspicious US features, and pathological reports should be conducted preoperatively to exclude parathyroid carcinoma. En bloc resection remains the gold standard of surgical approach for parathyroid carcinoma. The initial surgical approach for parathyroid carcinoma should involve an en bloc resection encompassing the parathyroid tumor along with the ipsilateral thyroid lobe, including the isthmus, as a single specimen. The key to the surgery is to avoid rupture of the tumor capsule to prevent implant metastasis [ ]. However, there is no doubt that the ablation needle will penetrate the capsule of the tumor and to some extent destroy the adjacent structure. Therefore, ablation is not suitable for parathyroid carcinoma.
- 2.
Parathyroid nodules that are difficult to access or located near critical structures (such as deep and/or parapharyngeal locations, adjacent to the recurrent laryngeal nerve (RLN) and/or esophagus) [ ].
- 3.
Abnormal vocal cord movement detected by laryngoscopy.
- 4.
Abnormal coagulation function test results.
- 5.
Patients with severe cardiopulmonary insufficiency who cannot tolerate thermal ablation.
Currently, thermal ablation therapy for parathyroid diseases is still in the research and development stage, and more clinical studies are needed to clarify its long-term efficacy and safety. When determining the treatment plan, we should fully respect the patient’s wishes and select the most appropriate treatment pathway based on individualized assessments. Additionally, we need to pay close attention to future research advancements to gain a more comprehensive understanding of the role of thermal ablation therapy in the management of parathyroid diseases.
Expert recommendation 13: Percutaneous thermal ablation is a potential alternative treatment to open surgery for benign parathyroid diseases, but strict adherence to the indications and contraindications is required. Recommendation level: IIa; Evidence level: B.
Q14: When multiple parathyroid glands are abnormal simultaneously, how to make a decision on ablation?
Expert opinion
The presence of multiple parathyroid abnormalities is generally observed in SHPT and can also be seen in THPT. A comprehensive preoperative US examination should be conducted to identify each parathyroid gland as much as possible. One or more PTGs were visualized in 75% of patients (144/192). They were visualized preferentially at the lower pole of the thyroid gland and in the infra-thyroid region (66%) [ ]. If the number of parathyroid glands displayed is less than four, it is necessary to combine the results of ECT imaging to observe for ectopic parathyroid glands. In this instance, the combination of other imaging methods such as 99mTc-MIBI, and PET/CT, can significantly improve the display rate of the parathyroid glands [ ]. If US can identify ≤ 3 parathyroid glands, the long-term efficacy of ablation is not good. If US can identify four parathyroid glands and the ablation needle access is safe, ablation therapy can be performed. During the ablation process, all four parathyroid glands need to be ablated, with three of them undergoing complete ablation and the largest one undergoing “near-total” ablation, which means initiating ablation when the ablation needle tip is 1 mm away from the distal capsule of the gland to preserve partial parathyroid function [ ].
For THPT, the basic principles are consistent with the ablation strategy for SHPT. Based on a comprehensive US assessment, all hyperplastic glands should be identified as much as possible in combination with ECT results. If ablation conditions are met, three of the parathyroids should be ablated as thoroughly as possible, while the smallest one should be left untreated.
Currently, there is no uniform standard regarding whether to perform single-session or multisession ablation. Given the minimally invasive and repeatable nature of thermal ablation, some studies suggest that for larger nodules or when there are ≥ 3 nodules, multisession ablation can not only improve treatment success rates but also effectively prevent postoperative hypocalcemia [ ]. Medical institutions can flexibly choose based on their own experience.
Expert recommendation 14: The primary aim of parathyroid ablation is to reduce the source of PTH. Preoperative assessment requires a balance between efficacy and complications. Recommendation level: I; Evidence level: B.
Q15: How to prevent injury of the recurrent laryngeal nerve (RLN) during ablation of parathyroid nodules?
Expert opinion
The superior parathyroid glands are located in close proximity to the cricothyroid membrane inlet of the RLN, and in cases of parathyroid adenoma or hyperplasia, downward displacement due to gravitational forces is relatively common. The inferior parathyroid glands exhibit greater positional variation, and larger inferior parathyroid glands may be situated dorsally to the RLN. The close anatomical relationship between the parathyroid glands and the RLN determines the objective possibility of RLN injury due to factors such as heat and mechanical compression during parathyroid ablation procedures.
Unilateral RLN injury may result in hoarseness, while bilateral injury can cause dyspnea or even asphyxia in patients. Therefore, preventing RLN injury is a crucial aspect of parathyroid ablation therapy. In previous studies, hydrodissection technique and lever separation technique are the most commonly used techniques to protect the RLN during ablation. The hydrodissection technique typically involves using a 18G or smaller PTC injection needle to inject sterile saline, sterile distilled water, or a 5% glucose solution between the parathyroid gland and nearby structures. This creates an isolation zone larger than 0.5 cm, effectively separating the parathyroid gland from the surrounding tissue. Since the RLN is difficult to precisely visualize via US intraoperatively, the injection site of the isolation fluid should be as close as possible to the parathyroid capsule to ensure effective nerve protection. Continuous supplementary injection of isolation fluid during the procedure is necessary to maintain the effectiveness of the isolation zone. For patients with inadequate liquid isolation, the lever separation technique can be used intraoperatively to pry the parathyroid gland away from surrounding critical structures, enhancing the safety of the surgery. Surgery should be approached with caution for patients in whom neither the hydrodissection technique nor the lever separation technique can effectively separate the parathyroid gland from surrounding tissues. A Meta-analysis has shown that the most common complication of parathyroid ablation therapy was transient vocal weakness or hoarseness, which usually resolved spontaneously within 6 months postoperatively without intervention, and permanent injury was rare. During the procedure, the patient’s voice should be monitored, and the plan for contralateral parathyroid surgery should be discontinued if any voice changes occur to avoid bilateral RLN [ ].
Expert recommendation 15: The hydrodissection technique is an important measure to prevent RLN injury during parathyroid ablation therapy. Recommendation level: I; Evidence level: B.
Q16: Does parathyroid disease require drug therapy before and after ablation?
Expert opinion
Currently, there is insufficient evidence-based medicine regarding the necessity of drug therapy before and after ablation for parathyroid lesions.
- 1.
Preablation treatment: According to the perioperative HPT management guidelines in China and other countries, patients with concurrent hypercalcemic crisis (serum calcium > 3.5 mmol/L) should treated with volume expansion, promotion of urinary calcium excretion, inhibition of bone resorption, or other treatments before surgery [ ]. For patients with vitamin D deficiency, vitamin D supplementation can be initiated at an appropriate dose preoperatively. Preoperative oral calcium and calcitriol can prevent or alleviate postoperative hungry bone syndrome. For patients not using calcitriol, initiating calcitriol at least 2 days before surgery can reduce the risk of severe hypocalcemia and decrease postoperative hospital stay and the need for intravenous calcium supplementation. In a study on parathyroid ablation, administering vitamin D supplements (at a dosage of 1000–2000 IU/day) to patients with vitamin D deficiency prior to the procedure and treating patients experiencing hypercalcemic crisis due to PHPT with intravenous fluid expansion or medications such as calcitonin, bisphosphonates, and furosemide resulted in good safety and efficacy of the ablation treatment [ ].
- 2.
Postablation therapy: Hypocalcemia is relatively common following parathyroid ablation therapy, and short-term supplementation of calcium and vitamin D can be administered to prevent hypocalcemia. Patients with vitamin D deficiency should continue to supplement vitamin D postoperatively. Hypocalcemia crisis is most likely to occur within 24h after secondary and tertiary parathyroid ablation. It is necessary to strengthen biochemical monitoring and timely supplement calcium, active vitamin D3 and its analogues to correct hypocalcemia.
Expert recommendation 16: Prior to parathyroid ablation, it is necessary to actively manage abnormalities in blood calcium levels. For patients with vitamin D deficiency, an appropriate amount of vitamin D supplementation can be initiated preoperatively. Recommendation level: IIa; Evidence level: C.
Q17: How to conduct standardized follow-up and efficacy evaluation after parathyroid ablation?
Expert opinion
Long-term follow-up is recommended after parathyroid ablation. The recommended follow-up times were 2h, 1d, 3d, 7d, 1 month, 6 months, 12 months after the operation, and then every 6 months thereafter [ , ]. Postoperative laboratory examination indicators include serum PTH, serum calcium, phosphorus, potassium, magnesium, and serum alkaline phosphatase (ALP). For abnormal indicators, continuous monitoring for 3 days is advisable.
Postoperative imaging examination preferably involves US, and CEUS can be combined when conditions permit. The outcomes of parathyroid ablation can be categorized into cure, persistent HPT, and recurrent HPT. [ ] For patients with PHPT, “cure” is defined as normalization of both serum calcium and PTH levels for more than 6 months. “Persistent HPT” refers to persistently elevated serum calcium levels 6 months after parathyroid ablation. “Recurrent HPT” is defined as normalization of serum calcium levels within 6 months after ablation, followed by the recurrence of hypercalcemia [ ]. For patients with PHPT who have normal serum calcium levels but persistently elevated PTH levels after ablation, the possibility of SHPT should be evaluated. [ ] For patients with SHPT, “persistent HPT” is defined as persistently elevated PTH levels after parathyroid ablation. “Recurrent HPT” is defined as PTH levels normalizing within at least 6 months after ablation and then gradually rising again [ ].
In addition, ECT imaging plays a crucial role in the follow-up of patients who have undergone parathyroid ablation. This imaging modality is particularly useful for assessing residual or recurrent parathyroid tissue, which may not be detectable by US and CEUS. ECT imaging is also helpful in monitoring the function of the parathyroid glands, especially in cases where there is a suspicion of persistent hyperparathyroidism or recurrence of the disease. By providing detailed information on the location and function of the parathyroid glands, ECT imaging aids in the planning of further interventions.
Expert recommendation 17: Follow-up after parathyroid ablation should include biochemical examination and imaging surveillance. US examination is the first choice for imaging, and CEUS and ECT can be combined if necessary. Recommendation level: I; Evidence level: B.
Q18: How to observe and deal with complications after parathyroid intervention?
Expert opinion
- 1.
RLN injury (0%–5.3%) [ , ]: The parathyroid glands are located in the cervical dangerous triangle, where the local anatomical structure is complex, and the glands are closely adjacent to the RLN. Intraoperatively, the patient’s vocalization can be used to assess whether the RLN is injured. If signs of RLN injury are present, ablation of contralateral lesions should be avoided. For intraoperative RLN injuries, immediate local injection of cold saline or isotonic glucose solution at around 25°C can be administered to reduce temperature and mitigate thermal damage. Additionally, the potential benefits of local or intravenous injection of dexamethasone should be considered. In the postoperative period, neurotrophic drugs can be administered orally. Hoarseness due to RLN injury typically resolves within 1 week to 6 months postoperatively, with some patients requiring 12 months or longer for recovery.
- 2.
Intraoperative bleeding (2.6%) [ ]: Minor bleeding generally requires no special treatment, but a large amount of bleeding leading to hematoma formation should be promptly addressed to prevent serious complications. Management options include: (a) pressure hemostasis, (b) US guidance to locate the bleeding point and use of the ablation needle for thermal coagulation to stop bleeding, (c) The use of a US-guided injection of hemostatic agents, such as thrombin, at the site of bleeding, and (d) the intravenous administration of hemostatic drugs. In general, prompt management of intraoperative hematoma can effectively stop bleeding, and the hematoma can be spontaneously absorbed postoperatively.
- 3.
Hypocalcemia (4.2%–22%) [ , ]: Hypocalcemia is a common complication of thermal ablation procedures. Besides symptoms such as limb numbness and spasms, hypocalcemia can also cause severe complications including bronchospasm, gastrointestinal spasms, seizures, and arrhythmias. Therefore, close postoperative monitoring of blood calcium levels and prompt treatment are crucial. Blood calcium levels should be monitored 2 to 4 times daily after the procedure. When blood calcium levels are below 2.11 mmol/L but above 1.8 mmol/L, oral calcium supplementation is administered. When blood calcium levels fall below 1.8 mmol/L, intravenous calcium supplementation is given [ , ].
- 4.
Hypoparathyroidism (0%–27.1%) [ ]: A small number of patients may have hypoparathyroidism, which may be caused by insufficient residual parathyroid glands or complete destruction of them during thermal ablation. This condition can be treated with oral calcium and active vitamin D supplements. Attention should be paid to the risk of kidney damage in the later stage [ , ].
Expert recommendation 18: Complications should be closely monitored and managed after parathyroid ablation, and the monitoring time should be determined according to the change of the patient’s condition. Recommendation level: I;Evidence level: B.
Q19: Should parathyroid cysts be observed or actively treated? Is sclerotherapy safe and effective?
Expert opinion
Parathyroid cysts are rare benign lesions occurring in about 0.1% to 0.3% of patients, usually found incidentally on imaging. The choice of treatment for parathyroid cysts should be based on whether the cyst is functional, its size, and the current clinical symptoms.
Nonfunctional parathyroid cysts can be initially observed. If the cyst is large enough to cause compression of surrounding tissues and produce clinical symptoms, percutaneous cyst aspiration and sclerotherapy can be considered. The treatment options for functional parathyroid cysts include surgical resection of the cyst, FNA of cyst fluid, or injection of sclerosing agents into the cyst [ , ]. Complete surgical resection is the preferred treatment method, which is related to the high concentration of PTH in the cyst fluid of functional cysts, which may cause parathyroid crisis in the case of rupture. Although FNA of cyst fluid is less invasive, its remission rate is only 33% with a high recurrence rate.
US-guided cyst sclerotherapy is commonly used for patients with compressive symptoms or those who strongly request treatment due to aesthetic concerns. In comparison to conventional surgical techniques, sclerotherapy presents a number of advantages, including a straightforward procedure, a high degree of reliability in terms of efficacy, minimal trauma, a reduced incidence of complications, and a limited impact on patients’ serum calcium, phosphorus, and parathyroid hormone levels. These attributes make it a suitable candidate for clinical promotion. Studies have shown that after sclerotherapy, cyst volume is significantly reduced, and serological indicators and clinical symptoms can be improved. However, there are also issues such as sclerosant leakage, damage to surrounding tissues and nerves, pain, and the possibility of requiring multiple sclerotherapy sessions [ ].
Expert recommendation 19: The treatment for parathyroid cysts should be selected based on their functionality, size, and symptoms, and sclerotherapy is a safe and effective treatment option. Recommendation level: IIa; Evidence level: C.
This Consensus Statements have some limitations. First, the issues in this consensus are mainly from the questionnaire survey, and the responses from the questionnaire survey cover only some of the areas, and the key concerns of the other areas are still unclear. Second, interventional treatment of parathyroid disease is not yet established in all regions, and to ensure the safety and effectiveness of the procedure, the operator must undergo rigorous training before performing the interventional technique. Third, long-term follow-up after parathyroid ablation has not been reported, and the necessary details of this technique may need to be further refined in the future.
Conclusions
This consensus, based on literature review and clinical experience, helps to diagnose and manage parathyroid disease. Although this consensus has been critically reviewed by the panel, it cannot be used as the sole criterion for the management of parathyroid disease and may need to be individually adjusted by physicians in a clinical setting.
Conflict of interest
The authors declare no competing interests.
Data availability statement
Data will be made available on request.
Acknowledgment
We sincerely acknowledge all the members and standing committee members of the Superficial Organs and Peripheral Vessels Committee, Chinese Association of Ultrasound in Medicine and Engineering. This paper may have some deficiencies. We welcome your valuable comments, which are very valuable to us. We will dedicatedly make corresponding modifications in future revisions. This work was supported by the National Key Research and Development Program of China ( 2023YFC2414203 ) and National Natural Science Foundation of China ( 82371972 ).
References
Related posts:
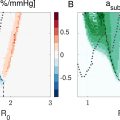 Ambient Pressure Sensitivity of Subharmonic Vibrating Single Microbubbles
Ambient Pressure Sensitivity of Subharmonic Vibrating Single Microbubbles
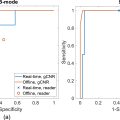 Comparative Assessment of Real-Time and Offline Short-Lag Spatial Coherence Imaging of Ultrasound Breast Masses
Comparative Assessment of Real-Time and Offline Short-Lag Spatial Coherence Imaging of Ultrasound Breast Masses
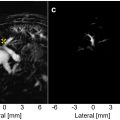 Hepatic Portal Venous Perfusion Imaging Using Vessel-Labeling Super-Resolution Ultrasound
Hepatic Portal Venous Perfusion Imaging Using Vessel-Labeling Super-Resolution Ultrasound
 The Potential for Blood–Brain Barrier Disruption During Transcranial Ultrasound Super-Resolution Imaging
The Potential for Blood–Brain Barrier Disruption During Transcranial Ultrasound Super-Resolution Imaging
 Delivering Gd-Labeled IgG Antibodies Into the Mouse Brain Following Focused Ultrasound Treatment
Delivering Gd-Labeled IgG Antibodies Into the Mouse Brain Following Focused Ultrasound Treatment
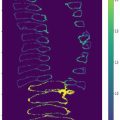 SSAT-Swin: Deep Learning-Based Spinal Ultrasound Feature Segmentation for Scoliosis Using Self-Supervised Swin Transformer
SSAT-Swin: Deep Learning-Based Spinal Ultrasound Feature Segmentation for Scoliosis Using Self-Supervised Swin Transformer
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


