Duodenal Polyps
Michael P. Federle, MD, FACR
Key Facts
Imaging
Duodenal polyps are much less common than gastric
Epithelial polyps (mucosal lesions)
Classified into 3 types
Adenomatous polyps (most common)
Single, lobulated or cauliflower-like surface
Hyperplastic polyps
Multiple, small, sessile polyps of uniform size
Hamartomas: Cluster of broad-based polyps
Can occur as part of Peutz-Jeghers syndrome
Submucosal (intramural) lesions
Duodenal GI stromal tumor (GIST)
Soft tissue density mass that deforms lumen
Lesions ≥ 2 cm often have central necrosis
Duodenal lipoma
Characteristic fat density on CT
Other mesenchymal tumors (rare)
Carcinoid tumor
Single or multiple; may ulcerate → “target” lesions
Top Differential Diagnoses
Brunner gland hyperplasia
Duodenal flexure pseudotumor
Ectopic gastric mucosa
Duodenal carcinoma
Intestinal metastases and lymphoma
Duodenal hematoma
Kaposi sarcoma
Ampullary carcinoma
Diagnostic Checklist
Check for family history of GI tract polyps
e.g., familial polyposis or Peutz-Jeghers
Lipomas can be diagnosed with confidence on CT
Most other polyps have nonspecific imaging features
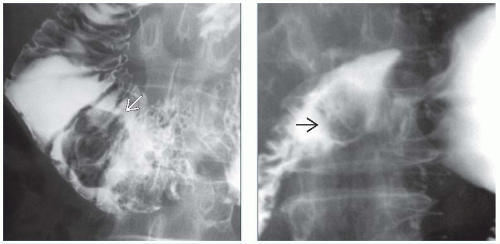 (Left) Upper GI series shows a large adenomatous polyp  as a radiolucent filling defect within the duodenum. (Right) Spot film from an upper GI series demonstrates a polypoid mass as a radiolucent filling defect within the duodenum. (Right) Spot film from an upper GI series demonstrates a polypoid mass  within the duodenal bulb. Endoscopic biopsy and resection revealed a hamartoma of the Brunner gland. Brunner gland hamartomas (hyperplasia) are usually multiple, smaller lesions. Larger, isolated lesions, as in this case, are indistinguishable from many other duodenal masses and require biopsy. within the duodenal bulb. Endoscopic biopsy and resection revealed a hamartoma of the Brunner gland. Brunner gland hamartomas (hyperplasia) are usually multiple, smaller lesions. Larger, isolated lesions, as in this case, are indistinguishable from many other duodenal masses and require biopsy. |
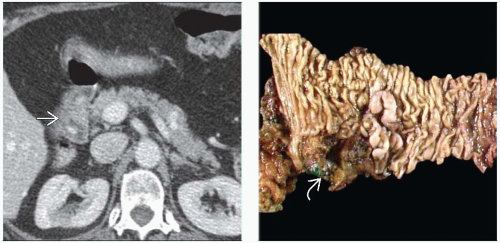 (Left) Axial CECT in a middle-aged man with vague abdominal pain shows a subtle heterogeneous mass  within the lumen of the 2nd part of the duodenum without signs of luminal obstruction. There was also no biliary or pancreatic ductal obstruction. (Right) Gross pathology in the same case shows the mass within the lumen of the 2nd part of the duodenum without signs of luminal obstruction. There was also no biliary or pancreatic ductal obstruction. (Right) Gross pathology in the same case shows the mass  previously identified on CT. After endoscopic confirmation of a villous tumor at this location, a pancreaticoduodenectomy (Whipple procedure) was performed. previously identified on CT. After endoscopic confirmation of a villous tumor at this location, a pancreaticoduodenectomy (Whipple procedure) was performed. |
TERMINOLOGY
Definitions
Protruding, space-occupying masses within duodenum
IMAGING
General Features
Best diagnostic clue
Radiolucent filling defects, ring shadows, or contour defect on barium study
CT signs of intraluminal &/or intramural mass
Size
Adenomatous and hamartomatous polyps: Several mm to 2 cm
Morphology
Epithelial polyps (mucosal lesions)
Adenomatous polyps (most common)
Usually single, lobulated or cauliflower-like surface
More evident on upper GI series than on CT
Hyperplastic polyps: Smooth, sessile, pedunculated
Much less common in duodenum than in stomach
Hamartomas: Cluster of broad-based polyps
Can occur as part of Peutz-Jeghers syndrome
General features
Duodenal polyps are much less common than gastric polyps
Polyps are classified into 3 types based on predominant glandular architecture
Adenomatous, hyperplastic, and hamartomatous
Adenomatous polyps
Most common polyps of duodenum
Are usually solitary
Unless part of polyposis syndrome
Typically arise from medial wall of bulb or 2nd part of duodenum
Increased risk of malignant change via adenomacarcinoma sequence
Composed of dysplastic epithelium
Depending on predominant glandular architecture, classified as
Tubular (75%), tubulovillous (15%), or villous (10%)
Duodenum: 2nd most common site of familial adenomatous polyposis (FAPS) after colon
Occur in 47-72% of familial polyposis cases
FAPS cases: Multiple sessile ± pedunculated polyps
Clustered around periampullary region
Also likely to have similar lesions in stomach
4% of patients develop periampullary carcinoma < 5 years after colectomy
Hyperplastic polyps
Rare, benign epithelial neoplasms of duodenumRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


