Abstract
Neuroendocrine carcinomas (NECs) of the esophagus are exceptionally rare, comprising only 0.04% of all neuroendocrine tumors. These malignancies can remain asymptomatic or manifest through digestive symptoms such as dysphagia and abdominal discomfort. Due to their rarity, limited studies exist, resulting in insufficient knowledge about their prognosis and treatment, with conflicting data in the literature.
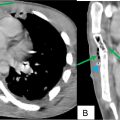
This report presents the case of a 62-year-old male chronic smoker with chronic dysphagia. Diagnostic evaluations, including gastroscopy and CT, revealed a circumferential lesion in the lower esophagus. Histopathological analysis confirmed a diagnosis of poorly differentiated large-cell neuroendocrine carcinoma.
Esophageal NECs are aggressive and poorly understood tumors. Tumor size, lymph node involvement, and metastatic status are critical factors influencing treatment decisions. However, there are no established guidelines for their management. Extensive research is urgently needed to develop standardized treatment approaches and improve the prognosis of patients with high-grade esophageal NECs.
Introduction
Neuroendocrine carcinomas (NEC) of the esophagus are extremely rare, as they represent 0.4% to 2% of all esophagus tumors [ ], and 0.04% of all neuroendocrine tumors [ ].
While the most commonly reported symptoms are dysphagia or abdominal discomfort, some tumors might be discovered incidentally during endoscopy.
With very few studies found in the literature, the knowledge surrounding NEC is reduced with the lack of standardized guidelines for its treatment and conflicting data regarding its prognosis [ ].
Due to improved diagnostic techniques, NEC have become an important diagnostic differential to consider, with incidence rates gradually increasing since 1970s [ ].
We report the case of a 62-year-old man, admitted for chronic dysphagia, to which the diagnosis of a NEC of the esophagus was retained.
Case presentation
A 62-year-old man, with history of chronic smoking for over 40 years, was admitted in our ward for chronic dysphagia.
He had a prolonged history of swallowing difficulties with multiple episodes of vomiting accompanied with a weight loss of 20 kgs in the last 6 months.
The patient also endorsed having early satiety, a reduced appetite and food regurgitation.
No family or personal history of neoplasm was found.
His initial vital signs were normal. The physical examination showed a cachectic body habitus with a nondistended abdomen. No hepatomegaly or large palpable gallbladder was palpable.
Other than a 3.3 mmol/l hypokalemia and a 132 mmol/l hyponatremia, routine blood and urine tests were normal.
The patient proceeded to an upper endoscopy, which revealed a hemi-circumferential ulcer-budding process in the lower part of the esophagus.
The biopsy revealed synaptophysin and CD56 immunostaining positive tumor (with a negative CK7 and P40) indicating poorly differentiated large cell neuroendocrine carcinoma ( Figs. 1 and 2 ).


Related posts:
 Breast cancer with medullary features shows a fast and plateau enhancement pattern on magnetic resonance images: A case report
Breast cancer with medullary features shows a fast and plateau enhancement pattern on magnetic resonance images: A case report
 A rare and life-threatening case of spontaneous hemopneumothorax presenting with severe hemodynamic instability
A rare and life-threatening case of spontaneous hemopneumothorax presenting with severe hemodynamic instability
 Primary sternal osteomyelitis in an immunocompetent adolescent
Primary sternal osteomyelitis in an immunocompetent adolescent
 Avascular necrosis of lateral femoral condyle in a middle-aged woman from central India
Avascular necrosis of lateral femoral condyle in a middle-aged woman from central India
 A very rare case of ileocolic and appendiceal intussusception with acute appendicitis
A very rare case of ileocolic and appendiceal intussusception with acute appendicitis
 An incidental finding of an ectopic intrauterine device (IUD) in the urinary bladder wall in a female presented with missed abortion
An incidental finding of an ectopic intrauterine device (IUD) in the urinary bladder wall in a female presented with missed abortion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


