Eventration and Paralysis of the Diaphragm
Michael P. Federle, MD, FACR
Mark M. Hammer, BS, MS
Key Facts
Imaging
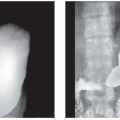
Eventration: Diaphragm muscle is thinned and permanently elevated but retains its continuity and attachments to costal margin
Partial: Most common, R > L
Anteromedial aspect of right hemidiaphragm, with space filled by liver
Paralysis: Lack of contraction of properly formed diaphragm muscle
Usually unilateral; bilateral is fatal
Unilateral may cause dyspnea
Best imaging tool: Sonography > fluoroscopy
US: Evaluates organs present in eventration
US: Evaluates diaphragm position and integrity
Paralysis usually has associated atelectatic lung (from paradoxical motion on inspiration)
CT valuable in some cases
Evaluate for differential diagnosis: Diaphragmatic hernia, peridiaphragmatic mass or fluid
Visualize eventration and its contents
Distinguish eventration from hernia, especially with multiplanar rendering
Liver or spleen “mushrooms” through site of eventration
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


