Abstract
The most prevalent thyroid cancer, known as papillary thyroid carcinoma, mainly affects those under 45 years of age, which is capable of metastasizing. It is more common for bone metastases to develop in the long bones, ilium, sternum, and scapula. Skull metastasis is common in lung, prostate, and breast carcinomas and, on the other hand, rare for thyroid carcinomas. Temporal bone as a site of metastasis is usually asymptomatic and uncommon. Isolated facial nerve palsy resulting from temporal bone metastasis is another rare phenomenon. Metastatic papillary thyroid carcinoma may have unusual manifestations, such as spinal cord compression due to bone metastases and palsy of the seventh cranial nerve. A 35-year-old female patient presented to the emergency department with gradual onset left-sided facial palsy, known to have a goiter. Nevertheless, she did not seek consultation until after experiencing left-sided facial weakness. On leading questions, the patient complained of weakness around the left eye, weakness around the angle of the mouth on the left side, left-sided earache, and hearing loss. The patient also complained of dysphagia, difficulty in breathing associated with excessive sweating, and a history of significant weight loss.Her CT neck and Neurological imaging were done, suggesting a solid lesion in the right lobe of the thyroid gland and a mass causing lysis of the left temporal bone and involvement of the facial nerve, respectively. A thyroid gland biopsy was taken and was suggestive of papillary thyroid carcinoma. It was later determined that the temporal mass was a metastatic papillary thyroid carcinoma follicular variant, which was eventually excised. In conclusion any patient presenting with isolated facial palsy with known case of thyroid disorder should be evaluated for malignancy as early diagnosis and treatment will limit the progression of the disease.
Introduction
Thyroid carcinoma is a rare disease, accounting for less than 1% of all new cancer cases [ ] . Ninety percent of thyroid tumors are differentiated thyroid carcinomas, which include both papillary and follicular subtypes. Differentiated thyroid carcinomas are often low-grade and slowly progressing. It is highly uncommon for differentiated thyroid carcinoma to spread to the base of the skull(including the temporal bone) [ ].
As far as we know, it has never been reported that papillary thyroid carcinoma spreads to the petrous part of the temporal bone. Owing to its infrequent occurrence and unique anatomical location, papillary thyroid carcinoma metastases to the base of the skull should always be ruled out with other skull base cancers.
Metastasis to the temporal bone is less frequently described than other bony metastases. Histopathologically, subclinical metastases to the temporal bone are more prevalent than previously considered. The age of occurrence spans between the young and the old [ ]. The most common sites for primary tumors are the breast and lung. Other common locations include the kidney, prostate, stomach, liver, and lung [ ]. The petrous part of the temporal bone is the preferred site of metastases, with as many as 82.9% found there compared to the mastoid and the internal auditory canal [ ]. The most prevalent mode of dissemination is hematogenous, as sluggish blood flow in the temporal bone promotes tumor cell deposition [ ].
Headache, vertigo, tinnitus, otalgia, otorrhea, and hearing loss are often observed as symptoms of temporal bone metastasis. Rarely they may exhibit facial nerve palsy.
We report a case of unilateral facial palsy associated with temporal bone tumor located in the petrous part of temporal bone. Initially suspected to be a benign skull based tumor, additional histopatholical and radiological studies revealed the cancer to be a metastatic follicular variant papillary thyroid carcinoma.
Case presentation
A 35-year-old female visited the hospital with complaints of left-sided facial weakness, which was gradual in onset and started with mild weakness on the left side of her face with difficulty in closing the eye or raising the eyebrow on the left side. It gradually progressed without specific aggravating or relieving factors ( Fig. 1 ). She also complained of dysphagia and difficulty in breathing associated with excessive sweating over the last few days. She also complained of left-sided earache and hearing loss. She had no known medical conditions other than the thyroid enlargement that had been there for the preceding 5 years, which grew in size over the years. Prior consultations for thyroid growth were nonexistent. She denied experiencing any past episodes of seizures, unconsciousness, behavior abnormalities, intense headaches, nausea, difficulty in walking, tinnitus, or otorrhea. Palpitations, tremors, and heat sensitivity were all denied by her.

On general examination, she was moderately built with a heart rate of 112 beats per minute, regular in rhythm and routine in volume, and a blood pressure of 130/90 mmHg in the right brachial artery taken in a supine position with no signs of pallor, icterus, cyanosis, clubbing, lymphadenopathy or edema.
A systemic evaluation found no evident abnormalities. A notable finding was peripheral or lower motor neuron facial paralysis on the left side, which did not include extra-ocular muscles. The face did not exhibit any sensory impairments. The rest of the cranial nerve examination was regular. The motor and sensory examination was also standard in the extremities.
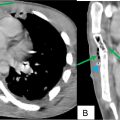
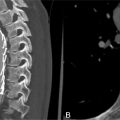
On local examination of the neck, there was an 8 × 6 cm hard mass on the front side that included the bilateral lobes of the thyroid gland, which was diffuse enlargement with no nodules. Routine and special blood tests indicated low TSH levels and high FT3 and FT4 levels(suggestive of hyperthyroidism) and raised serum thyroglobulin levels suggestive of probable differentiated thyroid carcinoma. The remainder of the laboratory investigations are shown in Table 1 .
| Parameter | Patients value | Normal value |
|---|---|---|
| Hemoglobin | 10.8 | 13-15 gm% |
| Red blood cells | 5.75 | 3.8-4.8 million/cu mm |
| White blood cells | 10,800 | 4000-10000 cu mm |
| MCV | 78.1 | 80-100 fl |
| Platelets | 1.77 | 1-5-4.0 lacks/cu mm |
| Hematocrit | 35% | 36%-46% |
| Aspartate aminotransferase | 24 | 14-36 u/l |
| Alanine aminotransferase | 19 | <35 u/l |
| Alkaline phosphatase | 86 | 38.126 u/l |
| Total bilirubin | 0.4 | 0.2-1.3 mg/dl |
| Albumin | 4.6 | 3.5-5.0 gm./dl |
| Globulin | 3.8 | 2.3-3.5 gm/dl |
| Urea | 26 | 7-17 mg/dl |
| Creatinine | 0.5 | 0.52-1.04 mg/dl |
| Sodium | 141 | 137-145 mmoL/L |
| Potassium | 3.8 | 3.5-5.1 mmol/L |
| Calcium | 7.9 | 8.4-10.2 mg/dl |
| Ferritin | 8.58 | 6.24-137ng/ml |
| CEA | 0.89 | <3 ng/ml |
| TSH | 0.013 | 0.465-4.68 mIU/ML |
| FT3 | 11.1 | 2.77-5.27 pg/ml |
| FT4 | 2.75 | 0.78-2.19 ng/ml |
| Serum thyroglobulin | 104 ng/mL | 3-40 ng/mL |
Related posts:
 Breast cancer with medullary features shows a fast and plateau enhancement pattern on magnetic resonance images: A case report
Breast cancer with medullary features shows a fast and plateau enhancement pattern on magnetic resonance images: A case report
 A rare and life-threatening case of spontaneous hemopneumothorax presenting with severe hemodynamic instability
A rare and life-threatening case of spontaneous hemopneumothorax presenting with severe hemodynamic instability
 Postextubation negative-pressure pulmonary edema after an appendectomy
Postextubation negative-pressure pulmonary edema after an appendectomy
 Primary sternal osteomyelitis in an immunocompetent adolescent
Primary sternal osteomyelitis in an immunocompetent adolescent
 Avascular necrosis of lateral femoral condyle in a middle-aged woman from central India
Avascular necrosis of lateral femoral condyle in a middle-aged woman from central India
 Hybrid imaging of a pseudoaneurysm of the descending thoracic aorta induced by a dorsal osteophyte: The silent killer
Hybrid imaging of a pseudoaneurysm of the descending thoracic aorta induced by a dorsal osteophyte: The silent killer
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


