Abstract
Purpose
In lung cancer patients, the distinction between synchronous primary lung cancer and intrapulmonary metastasis can be challenging. The intensity of FDG uptake in pulmonary lesions has been shown to be potentially useful in classifying synchronous lung cancer. The aim of this retrospective study is to investigate the effectiveness of FDG uptake in differentiating metastases from synchronous primary lesions in the setting of lung cancer.
Methods
Consecutive patients with primary lung cancer with two or more malignant lung lesions referred for ( 18 F)-FDG PET-CT imaging between 2010 and 2019 were reviewed and classified into synchronous and metastasis groups. Lesional maximum standardized uptake values (SUV max ), relative differences in SUV max and SUV max ratios were calculated and compared using receiver operating characteristic (ROC) curve analysis. Intra-group correlation in SUV max between lesion pairs was examined using Pearson’s and Spearman’s correlation analysis.
Results
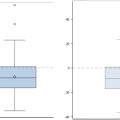
94 patients were included for analysis, divided into synchronous ( n = 62; 68 lesion pairs) and metastasis ( n = 32; 33 lesion pairs) groups. The correlation of FDG uptake between lesions in the metastasis group was strong ( r = 0.81). A significant difference in mean relative difference in SUV max (synchronous: 0.50±0.23 metastasis: 0.34±0.17, p = 0.001) and mean SUV max ratio (synchronous: 2.6 ± 1.7 metastasis: 1.7 ± 0.6, p < 0.001) was observed. ROC analysis revealed a fair AUC (0.71–0.72) for these parameters, with an associated sensitivity of 59 % and specificity of 82 % at optimal cut-off values.
Conclusion
Differences in FDG uptake intensity among multiple synchronously presenting malignant nodules may be helpful to distinguish second primary lung tumours from metastatic spread.
1
Introduction
Fluorine-18 fluorodeoxyglucose positron emission tomography-computed tomography (F)-FDG PET-CT) imaging is routinely performed for initial staging of primary lung cancer, which assesses the glucose metabolism of tumors [ , ]. In patients with more than one hypermetabolic lung lesion suspected to be malignant, the lung lesions could represent either synchronous primary lung cancers or a primary cancer with metastatic spread . According to the American Joint Committee on Cancer (AJCC) cancer staging system , tumors may be considered second primaries if they are clearly of a different histologic type on biopsy. Based on time of presentation, multiple discrete tumours may further be designated as synchronous (if an additional tumour appears within 6 months of an initial index tumour) or metachronous (if a new tumour emerges beyond this timepoint) . The gold standard for differentiation includes immunohistochemistry and P53 gene mutation analyses [ , ], which may not be routinely performed or feasible.
In cases of equivocal histopathological findings or in situations where patients are unable to tolerate a biopsy or it being infeasible due to lesion location, FDG PET-CT may be helpful. The criteria favoring separate tumors include differences in radiological appearance or metabolic uptake on FDG PET-CT . In addition, it may be easier to differentiate two primary cancers if they have different histopathology. The challenge is when tumors show similar histopathological features wherein it remains difficult to determine whether the tumor is a second primary lung cancer or a metastasis.
The distinction of synchronous primary lung cancer from intrapulmonary metastasis affects staging and management, underlying its clinical significance. If the second lesion represents metastasis, TNM staging based on the 8th edition of the AJCC staging system classifies a separate tumor in a different lobe of the ipsilateral lung as T4 (stage III) while a tumor in the contralateral lung is considered as M1a (stage IV) . Patients with lung metastases may not be suitable surgical candidates and thus, are typically treated with palliative intent . In contrast, aggressive surgical intervention has been proven to be safe and effective in patients with synchronous primary lung carcinoma and negative nodal involvement [ , ].
Standardized uptake value (SUV) is a semiquantitative measure of FDG uptake, which serves as a proxy for tumor metabolic activity. It is known that poorer tumour differentiation and higher tumour aggressiveness correspond to higher FDG uptake . It has also been shown that the difference in FDG uptake between two lung nodules could be helpful in differentiating metastatic disease from second primary tumours in patients with synchronously presenting pulmonary lesions [ , ].
Tumours with a shared clonal origin often behave similarly and have common histological features. We hypothesized that the SUVs of clonally related tumours (i.e., metastases) would be more similar in FDG uptake than tumours possessing a different clonal origin, and, consequently, that a larger difference in FDG uptake would potentially infer the presence of synchronous primary lung cancers rather than metastatic disease. The primary objective of the study is to assess the diagnostic value of FDG uptake intensity for differentiating synchronous lung cancer from metastasis in patients with multiple malignant lung lesions. The secondary objective is to assess the correlation of FDG uptake parameters of lung lesions between the synchronous and metastasis patient groups.
2
Materials and methods
2.1
Study design
A single-centre retrospective study was performed to examine the use of maximum SUV (SUV max ) parameters to reliably distinguish between second primary lung tumours and lung metastases in the setting of primary lung cancer. For the purposes of this study, two groups were defined, analyzed, and compared: the “synchronous group”, representing patients presenting with multiple primary lung cancers, and the “metastasis group”, representing patients presenting with intrapulmonary metastasis from a primary lung cancer.
2.2
Patients
Consecutive patients with lung cancer (confirmed or suspected) referred for FDG PET-CT imaging between January 2010 to December 2019 with two or more hypermetabolic lung nodules were included. Most patients were referred for diagnosis and initial staging. Patients with prior treatment for lung cancer were excluded and therefore only patients for initial staging were included. In addition, patients with tumours of unknown or uncertain clonal origin, small lesion sizes (<8 mm), ground glass opacities, metastases from extrapulmonary malignancies, and active inflammatory or infectious conditions were excluded.
2.3
18 F-FDG PET data acquisition and reconstruction
All patients underwent whole-body FDG PET-CT imaging as part of their routine preoperative staging procedure. Before FDG administration, patients fasted for 6 h. Patients’ glucose level was subsequently verified (≤9.0 mmol/L was considered acceptable before 2015, which was relaxed to 11.0 mmol/L based on the current guidance document ). Images were acquired at 60 min following radiotracer administration.
FDG PET images were acquired with the GE Discovery 710 Scanner (GE Healthcare) after administration of 2-( 18 F)-fluoro-2-deoxy- d -glucose with three-dimensional (3D) acquisition. The administered dose was weight-based (5 MBq/kg) and the spatial resolution of the PET scanner was 5 mm. Images were acquired over 2.5 min intervals per bed position using typical image acquisition parameters on the GE Discovery 710 PET-CT scanner. Images were reconstructed by ordered subset expectation maximization (OSEM) with correction for attenuation and scattering on the GE Discovery 710 scanner and subsequently interpreted on HERMES workstation. For each pulmonary nodule, the SUV max (defined as the maximum uptake value of a lesion taken as the voxel with the highest activity level within the volume of interest) was measured by a nuclear medicine fellow and subsequently verified by a nuclear medicine physician with 20 years of FDG PET experience.
2.4
Histopathological data
A tumour was considered a second primary tumour if histopathological or immunohistochemical features differed from those of the index tumour, demonstrating separate clonal origin. The relevant pathology report was accessed and reviewed from each patient’s chart in the hospital and provincial electronic medical record. Patients without conclusive diagnosis of second primary cancer due to the impossibility of gaining adequate tissue samples for confirmation were excluded. Metastatic disease was concluded based on identical histopathological findings and immunohistochemical staining of the lesions pointing toward a shared clonal origin or clinical suspicion involving tumour morphological and spatial characteristics consistent with metastatic spread (metastasis group). In patients with multiple primary lung cancers, further distinguishing between synchronous and metachronous lesions (based on aforementioned differences in time of lesion detection) is difficult due to the lack of sequential imaging studies. For simplicity, we grouped these patients together (synchronous group).
2.5
Statistical method
In addition to SUV max , the absolute difference in SUV max (∆SUV max ) between hypermetabolic pulmonary nodules was calculated in each patient, where SUV max 1 corresponded to the lesion with the higher uptake value (∆SUV max = SUV max 1 – SUV max 2 ). Relative difference in SUV max (relative ∆SUV max ) was calculated using ∆SUV max relative to SUV max 1 (∆SUV max /SUV max 1 ), while SUV max ratio was expressed in terms of SUV max 1 to SUV max 2 . In the case of patients presenting with more than two synchronous lung lesions, pairwise comparisons were conducted for all possible permutations in the synchronous group such that the SUV max of the less FDG-avid lesion was subtracted from the SUV max of the more FDG-avid lesion. For instance, in a patient presenting with 3 synchronous pulmonary nodules, the values SUV max 1 , SUV max 2 and SUV max 3 were recorded, and the differences in SUV max were calculated as ∆SUV max = SUV max 1 – SUV max 2 , SUV max 1 – SUV max 3 and SUV max 2 – SUV max 3 (where SUV max 1 > SUV max 2 > SUV max 3 ). In the metastasis group, pairwise comparisons were conducted using the primary tumour as the index tumour 1, which was taken as the lesion with the highest SUV max measurement, where ∆SUV max = SUV max 1 – SUV max 2 .
The imaging parameters between the synchronous and metastasis groups were analysed using the Mann–Whitney U test as none of the parameters followed a normal distribution based on the Shapiro-Wilk test. Correlation of FDG PET uptake (given by SUV max measurements) between lesion pairs in the metastasis group (expected linear relationship) was performed by Pearson’s analysis and the synchronous group (expected non-linear relationship) was examined using Spearman’s correlation analysis. For discrete histopathological types, receiver operating characteristic (ROC) analysis was performed to determine the area under the curve (AUC), optimal cut-off value, and corresponding sensitivity and specificity of SUV max ratio and relative difference in SUV max as suitable parameters to differentiate between second primary lung tumours and metastasis. All statistical tests were two-tailed and a p- value below 5 % was considered statistically significant. All analyses were performed with IBM SPSS Statistics (version 26, IBM, USA).
3
Results
3.1
Patient distribution
Upon reviewing patient chart records, a total of 577 patients with two or more hypermetabolic lung lesions were identified. After exclusion of patients with lesions of unknown or uncertain tumour histopathology ( n = 439), small lesion size ( n = 9), ground glass opacity appearance ( n = 9), and metastatic disease originating from extrapulmonary tumours ( n = 26), 94 patients (age: 69±9, F: M = 55:39) remained for analysis. Of those patients, 62 patients comprised the synchronous group, where 59 patients had two lesions and three patients had three lesions, with all lesions confirmed by histopathology to be of different clonal origin and thus, represented separate primary lung tumours. In terms of histological subtype, the majority of lesions represented adenocarcinoma (43 of the first lesions and 52 of the second lesions), followed by squamous cell carcinoma (15 of the first lesions and 7 of the second lesions). The metastasis group, consisting of 32 patients, was further sub-divided based on whether the metastatic tumour was confirmed by histopathology ( n = 11) or suspected due to imaging features and clinical information suggesting metastatic disease ( n = 21) ( Fig. 1 ). One patient in the metastasis group had two biopsy-proven metastases. In contrast to the synchronous group, a larger proportion of lesions corresponded to squamous cell carcinoma in the metastasis group, followed by adenocarcinoma and others.

3.2
Tumour characteristics
In comparing nodule size between the two lesions in each patient, the first lesion was taken as the one with the more intense FDG uptake. The mean lesion volume of the two lesions in the synchronous group was 23 ml (±45 ml) and 5 ml (±13 ml), while the mean volume of the two lesions was 59 ml (±63 ml) and 4 ml (±7 ml) in the metastasis group. In terms of nodule distribution, the majority of metastatic tumours (84 %) were found in the same lobe as the primary cancer whereas second primary tumours tended toward a more variable distribution pattern, with only 20 % of tumours presenting in an intra-lobar manner.
3.3
Tumour SUV parameters
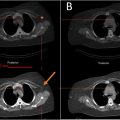
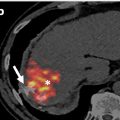
For the synchronous group, mean SUV max was 11.6 ± 7.4 for lesion 1 and 5.0 ± 3.0 for lesion 2, and for the metastasis group it was 14.2 ± 6.9 for lesion 1 and 9.0 ± 4.5 for lesion 2 ( Table 1 ). The difference in FDG uptake in both index (SUV max 1 ) and second lesions (SUV max 2 ) between the synchronous and metastasis groups was significant ( p = 0.026 for the index lesion and p < 0.001 for the second lesion). Representative cases from the synchronous and metastasis groups with imaging results and FDG uptake values are shown in Fig. 2 .
Related posts:
 Feasibility of deep learning-reconstructed thin-slice single-breath-hold HASTE for detecting pancreatic lesions: A comparison with two conventional T2-weighted imaging sequences
Feasibility of deep learning-reconstructed thin-slice single-breath-hold HASTE for detecting pancreatic lesions: A comparison with two conventional T2-weighted imaging sequences
 Non-visualization of axillary pathological lymph nodes in breast cancer patients on SPECT/CT and during operation
Non-visualization of axillary pathological lymph nodes in breast cancer patients on SPECT/CT and during operation
 Development of a deep learning model for the automated detection of green pixels indicative of gout on dual energy CT scan
Development of a deep learning model for the automated detection of green pixels indicative of gout on dual energy CT scan
 Addition of contrast in ultrasound screening for hepatocellular carcinoma
Addition of contrast in ultrasound screening for hepatocellular carcinoma
 Combination of intrahepatic TARE and extrahepatic TACE to treat HCC patients with extrahepatic artery supply: A case series
Combination of intrahepatic TARE and extrahepatic TACE to treat HCC patients with extrahepatic artery supply: A case series
 Impact of inspiration level on lung nodule volumetry
Impact of inspiration level on lung nodule volumetry
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


