Abstract
A 43-year-old female was admitted with a 1-month history of recurrent periumbilical abdominal pain and nausea. The patient had a 7-year history of Azathioprine use for the management of myasthenia gravis with AChR antibodies. The initial abdominal ultrasound revealed thickened small bowel walls at multiple sites. Abdominal CT enterography (CTE) raised suspicion for Crohn’s disease or lymphoma. Upper gastrointestinal endoscopy revealed multiple ulcers in the gastric body and antrum, with biopsy samples taken from the lesions. Histopathological analysis confirmed a diagnosis of B-cell lymphoma in the stomach. However, the imaging characteristics of the small bowel lesions on CTE were inconclusive in distinguishing between Crohn’s disease and lymphoma. After a multidisciplinary discussion, the patient was indicated for chemotherapy based on the confirmed diagnosis of gastric lymphoma. While awaiting the scheduled chemotherapy session, the patient developed sudden right iliac fossa pain, which subsequently spread across the abdomen. CT imaging revealed a perforation of the small intestine in the right iliac fossa. The patient underwent surgical resection of the affected small bowel segment, and pathological examination confirmed B-cell lymphoma in the small intestine.
Introduction
Gastrointestinal (GI) lymphoma is the most common form of extranodal lymphoma with the majority being non-Hodgkin type. Immunosuppressive therapies, such as Azathioprine (AZA), have been widely recognized for their role in increasing the risk of lymphoma [ ]. This connection is particularly well-documented in individuals undergoing organ transplantation and other immunosuppressed populations, highlighting the potential consequences of prolonged immunosuppression [ , ]. The clinical symptoms and imaging features of GI lymphoma are nonspecific and can sometimes be difficult to distinguish from inflammatory bowel diseases such as Crohn’s disease, potentially leading to delayed treatment. We report a case of multifocal lymphoma in the stomach and small intestine in a patient with a history of prolonged Azathioprine treatment, featuring imaging characteristics that mimic Crohn’s disease.
Case presentation
A 43-year-old female patient presented to our hospital with complaints of recurrent abdominal pain, nausea, and vomiting without fever lasting for 1 month. History of myasthenia gravis with AChR antibodies, treated with azathioprine for 7 years. No history of surgery. No notable family medical history. Physical examination findings: stable vital signs, tenderness in the right iliac fossa, no signs of guarding. Hematological findings: Leukocyte count within normal limits, no neutrophil predominance, mild elevation of C-reactive protein (CRP) at 19.3 mg/L, and normal procalcitonin levels. Molecular biology testing was performed to detect gastrointestinal pathogens, including 7 bacteria: Shigella spp./EIEC, Campylobacter spp., Yersinia enterocolitica, Vibrio spp., Clostridium difficile toxin B, Aeromonas spp., and Salmonella spp . All results were negative. The automated immunoassay results for CMV, EBV, and amebiasis indicate no signs of acute infection. Calprotectin in stool: 447 µg/g. The initial ultrasound images revealed thickening of the small intestinal wall at multiple locations, with signs of small bowel intussusception in the left iliac fossa, but no indications of bowel obstruction were observed. The patient subsequently underwent CTE for further evaluation of suspected pathology. Since the patient did not present with symptoms of bowel obstruction and the initial ultrasound indicated small bowel lesions, we opted for a CTE scan instead of a conventional abdominal-pelvic CT scan to achieve a more comprehensive evaluation of the small intestine.
Imaging findings
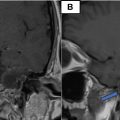
CTE was performed using a 128-slice MSCT scanner with intravenous contrast in the enteric phase (45 seconds) to optimally assess the enhancement characteristics of the small intestine. The plain sequence images were used to ensure adequate distension of the small bowel loops. CTE provides detailed imaging findings of small bowel and mesenteric pathology that are not easily accessible via endoscopy. Skip lesions were observed in multiple segments of the jejunum and ileum, along with involvement of the greater curvature of the stomach. There was marked thickening of the gastric mucosal folds. Small bowel wall thickening was noted, with a maximum thickness of approximately 15 mm. Most loops demonstrated symmetric wall thickening with homogeneous contrast enhancement over an extended segment, while a few loops exhibited asymmetric wall thickening, predominantly involving the mesenteric border, as shown in Figs. 1 and 2 . Additionally, pseudoaneurysmal dilatation was present in the ileal loop located in the right iliac fossa. Imaging also revealed small bowel-small bowel intussusception in the left iliac fossa, characterized by thickened and homogeneously enhancing bowel walls at the lead point, without any signs of bowel obstruction. No regional lymph node enlargement was observed, and no hepatic or splenic lesions were identified. Furthermore, there was no evidence of fistula or abscess formation in the abdominal cavity.


The described imaging findings are consistent with small bowel lymphoma. However, due to the asymmetric wall thickening, predominantly involving the mesenteric border, which is considered a specific sign of Crohn’s disease, this diagnosis cannot be ruled out.
As CTE detected lesions in the stomach, the patient was indicated for gastroscopy to assess the lesions and perform a biopsy. In this case, CTE could not differentiate between intestinal lymphoma and Crohn’s disease, so the patient was also indicated for colonoscopy for diagnostic purposes. Colonoscopy and terminal ileoscopy showed no pathological findings. Gastroscopy revealed multiple superficial ulcers in the gastric corpus, and a biopsy was performed on the gastric lesion. Histopathological results confirmed gastric B-cell lymphoma ( Fig. 3 ).

Related posts:
 A rare and life-threatening case of spontaneous hemopneumothorax presenting with severe hemodynamic instability
A rare and life-threatening case of spontaneous hemopneumothorax presenting with severe hemodynamic instability
 A very rare case of ileocolic and appendiceal intussusception with acute appendicitis
A very rare case of ileocolic and appendiceal intussusception with acute appendicitis
 Petrous apex epidermoid cyst: A rare case
Petrous apex epidermoid cyst: A rare case
 Successful endovascular treatment for pediatric ruptured cervical spinal perimedullary arteriovenous fistula: A case report
Successful endovascular treatment for pediatric ruptured cervical spinal perimedullary arteriovenous fistula: A case report
 Corrigendum to “Intracranial mesenchymal tumor with multiple extracranial metastases: a case report and literature review.” [Radiol Case Rep, 2024;19(2):825–830]
Corrigendum to “Intracranial mesenchymal tumor with multiple extracranial metastases: a case report and literature review.” [Radiol Case Rep, 2024;19(2):825–830]
 Persistence of the hypoglossal artery: A rare case report
Persistence of the hypoglossal artery: A rare case report
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


