Gastrointestinal System
QUESTIONS
1 What radiotracer is commonly used for the following exam that was done for the evaluation of gastroparesis?
 |
A. Tc-99m pertechnetate
B. Tc-99m sulfur colloid
C. Tc-99m mebrofenin
D. Tc-99m dimercaptosuccinic acid (DMSA)
View Answer
1 Answer B. For the evaluation of gastroparesis, approximately 1 mCi of Tc-99m sulfur colloid (SC) is cooked with 4 oz of egg white or whole egg and served with 2 slices of bread, 30 g of strawberry jam and 120 mL of water. Tc-99m SC remains bound to the ovalbumin in the egg white and does not dissociate into the liquid when in the stomach, thus allowing for accurate measurement of the solid emptying. If the patient is allergic to eggs, oatmeal can be used. Measuring simultaneous solid and liquid emptying is feasible by a dual isotope study using an In-111 diethylenetriamine pentaacetic acid (DTPA)-radiolabeled liquid and Tc-99m SC-labeled solid. Tc-99m mebrofenin is used for the hepatobiliary scintigraphy. Tc-99m pertechnetate is typically used for salivagram in infants, for thyroid scintigraphy, or for the evaluation of Meckel diverticulum. Tc-99m dimercaptosuccinic acid (DMSA) is typically used for renal cortical imaging.
References: Abell TL, Camilleri M, Donohoe K, et al. Consensus recommendations for gastric emptying scintigraphy: a joint report of the American Neurogastroenterology and Motility Society and the Society of Nuclear Medicine. Am J Gastroenterol 2008;103(3):753-763.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:294-305.
2 Which medication should be discontinued 48 to 72 hours before gastric emptying scan?
A. Labetalol
B. Ondansetron
C. Morphine
D. Oral hypoglycemic
View Answer
2 Answer C. Opiate analgesic medications (e.g., morphine, codeine, Demerol, and oxycodone) calcium channel blockers, antacids, and anticholinergic agents delay gastric emptying (GE); they can result in a false-positive study if not discontinued for the appropriate amount of time prior to the examination. Prokinetics such as domperidone may lead to a false-negative GE study in a patient with gastroparesis and should be stopped before the study as well. Serotonin receptor (5-HT-3) antagonists, such as ondansetron, have little effect on GE and may be given for severe symptoms of nausea and vomiting before the GE study. Insulin-dependent diabetics should be scheduled for an early morning study and should generally take 1/2 of their usual morning insulin dose, followed by the radiolabeled meal. Patients on oral hypoglycemic should be instructed to take their usual morning dose of hypoglycemic medication shortly before the radiolabeled meal. Since hyperglycemia may delay gastric emptying independently, the study should be rescheduled if the fasting blood glucose level is >200 mg/dL.
Reference: Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:295, 297.
3 Which of the following counts are preferred to generate the time activity curve in the gastric emptying study?
A. Anterior
B. Posterior
C. Geometric mean
D. Left anterior oblique
View Answer
3 Answer C. For gastric emptying study, anterior and posterior planar images with the distal esophagus, stomach, and proximal small bowel in the field of view should be obtained for 1 min immediately after ingestion of the meal and at 1, 2, and 4 hours on the same camera. Anterior and posterior views allow for the calculation of the geometric mean (GM) using the following formula: geometric mean = square root (anterior counts × posterior counts). GM more accurately represents the amount of tracer in the stomach since it accounts for posterior-to-anterior movement of the food as it travels from the fundus to the antrum, thus allowing for mathematical attenuation correction. Anterior and posterior data are obtained simultaneously with a dual-head gamma camera or sequentially on a single-headed camera. As the half-life of Tc-99m sulfur colloid is 6 hours, all data must be corrected for radioactive decay. While counts from left anterior oblique (LAO) projection can be used as an alternative to GM, GM is the more accurate and preferred method of the two.
Reference: Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:304.
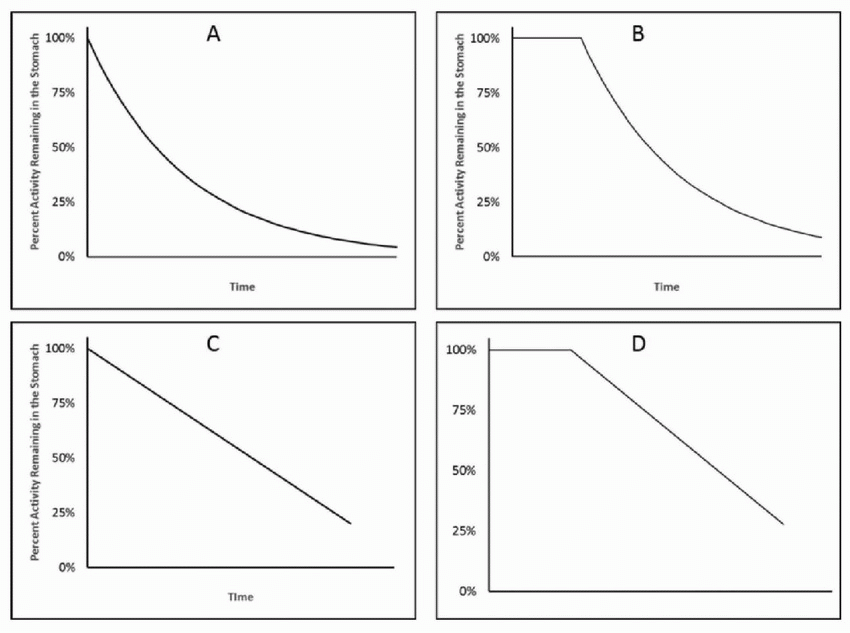
4 Which of the following curves most likely represents normal emptying of the liquids from the stomach?
 |
View Answer
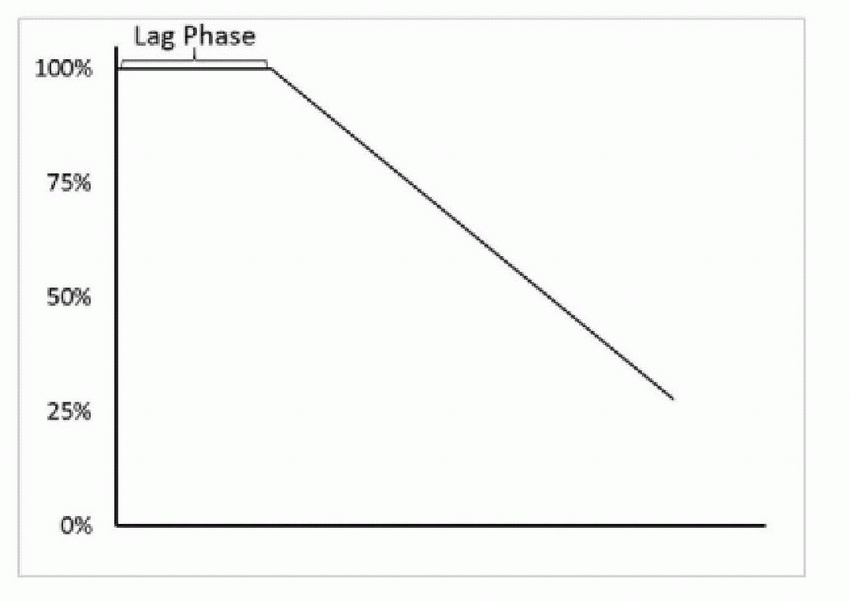
4 Answer A. Liquid normally empties from the stomach in a monoexponential pattern soon after it enters the stomach as shown by the curve in choice A. On the other hand, ingested solid food gets converted into smaller particles (chyme) by mechanical grinding and by chemical digestion before it begins to empty from the stomach. The length of time required for this to occur is referred to as the lag phase, a period of time when there is no significant emptying of the solids from the stomach. It usually lasts for 5 to 20 minutes. Once initiated, the emptying of the solid food from the stomach normally occurs in a linear fashion. As such, a normal solid gastric emptying curve would look like that seen on choice D.
 |
References: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:264-267.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:295.
5 Where in the liver does the Tc-99m sulfur colloid localize?
A. Hepatocytes
B. Sinusoids
C. Kupffer cells
D. End arterioles
E. Bile canaliculi
View Answer
5 Answer C. The average particle size of the Tc-99m sulfur colloid (SC) is about 0.3 to 1.0 µm. Given its particulate nature, Tc-99m SC is phagocytosed by the reticuloendothelial system: Kupffer cells in the liver and macrophages in the spleen and bone marrow.
Reference: Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:307-314, 161.
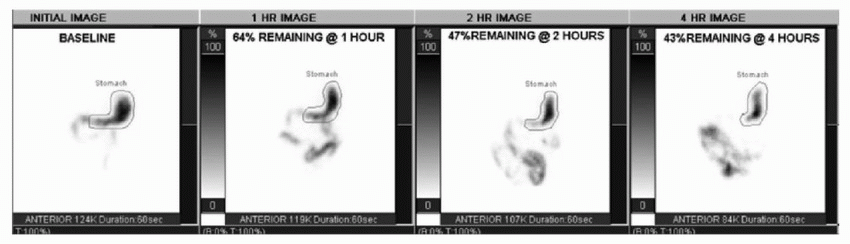
A. Normal gastric emptying
B. Gastroparesis
C. Gastric hypermotility
D. Gastroesophageal reflux
View Answer
6 Answer B. Normal values for the standardized solid meal gastric emptying study are shown in the table below. Forty-three percent remaining activity in the stomach at 4 hours suggests gastroparesis. The 4-hour time point is more sensitive for detection of delayed gastric emptying compared to the 2-hour time point. In this patient, 47% remaining at 2 hours would have been normal and the diagnosis of gastroparesis would have been missed if 4-hour imaging was not acquired. Gastric hypermotility is suggested if there is <30% retention at 1 hour (>70% emptying).
Normal Values for Standardized Solid Gastric Emptying Study | ||
Time | % Gastric Retention | % Gastric Emptying |
1 h | <90 but > 30% | >10 but <70% |
2 h | <60 | >40 |
4 h | <10 | >90 |
References: Abell TL, Camilleri M, Donohoe K, et al. Consensus recommendations for gastric emptying scintigraphy: a joint report of the American Neurogastroenterology and Motility Society and The Society of Nuclear Medicine. Am J Gastroenterol 2008;103(3):753-763.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:294-305.
7 In a tagged red blood cell (RBC) scan, where does the Tc-99m bind in the red blood cells?
A. Alpha chain of the hemoglobin
B. Beta chain of the hemoglobin
C. Gamma chain of the hemoglobin
D. Delta chain of the hemoglobin
View Answer
7 Answer B. Tc-99m pertechnetate binds to the beta chain of the hemoglobin molecule.
Reference: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:183.
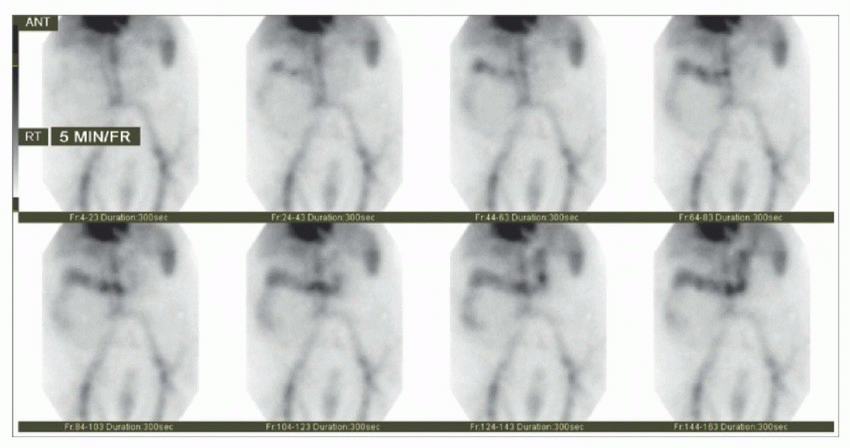
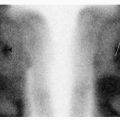
8 In the following patient with an acute gastrointestinal bleed, a branch supplied by which of the following major vessels is the most likely source of bleeding?
 |
A. Celiac artery
B. Gastroduodenal artery
C. Superior mesenteric artery (SMA)
D. Inferior mesenteric artery (IMA)
View Answer
8 Answer C. Since the gastrointestinal (GI) bleeding can be an intermittent process, tagged red blood cell (RBC) study helps identify patients who are bleeding at time of exam (thus suitable for angiography) and helps localize the probable site of bleeding. Dynamic acquisition and review of images in the cine mode allows for better localization and increased sensitivity. GI bleeding is marked by (1) accumulation of radiolabeled RBCs outside the normal area of vascular blood pool, (2) increasing intensity over time, and (3) movement within the bowel either in an antegrade or in a retrograde direction. At 10 minutes (frame 2), a focal uptake in the hepatic flexure is seen, which increases in intensity over time, conforms to the large bowel, and moves in the antegrade and retrograde directions. This area is typically supplied by the superior mesenteric artery (SMA). The SMA supplies the bowel from the second portion of the duodenum as far distally as the splenic flexure of the transverse colon. The celiac artery supplies the distal esophagus, stomach, and the 1st portion of the duodenum. The inferior mesenteric artery (IMA) supplies from the distal third of the transverse colon to proximal rectum. Accurate localization of GI bleeding on tagged RBC study helps direct the interventional radiologist to a specific vascular territory. This allows for prompt localization, reducing the procedure time and patient radiation exposure. Quick localization should also minimize the chance that intermittent bleeding would have stopped by the time of contrast injection.
References: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:245-248.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:307-314.
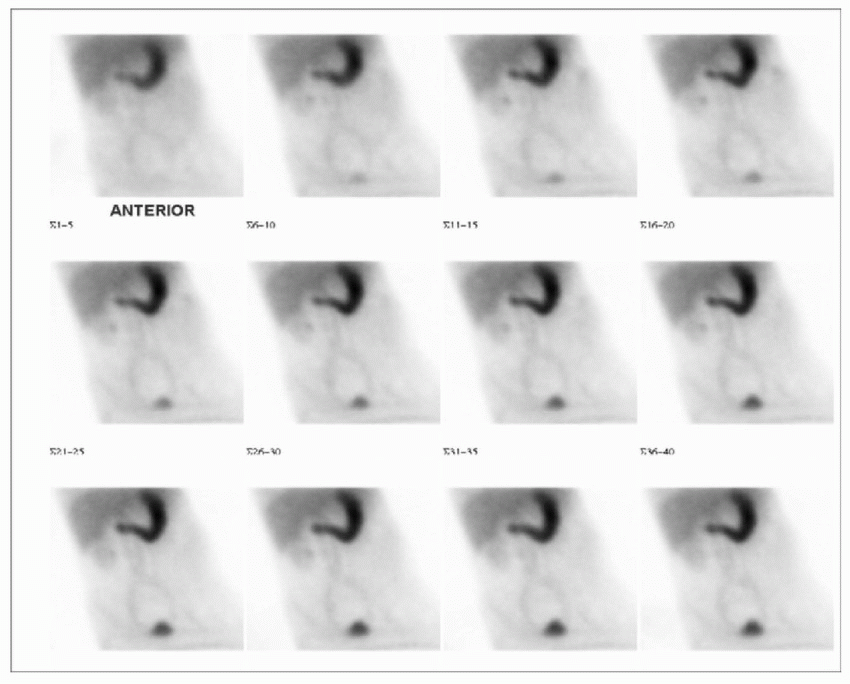
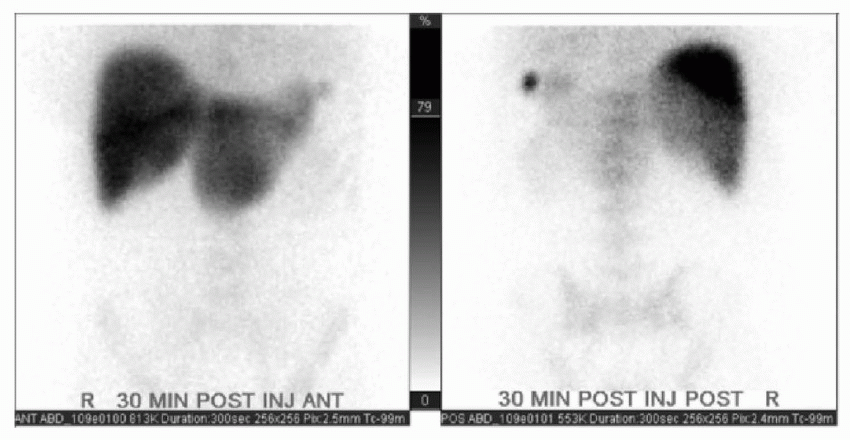
9 The following image is from a patient who underwent Tc-99m RBC scintigraphy for the evaluation of gastrointestinal bleeding. What is the MOST likely diagnosis?
 |
A. Bleeding gastric ulcer
B. Severe gastritis
C. Enterogastric reflux
D. Free pertechnetate
E. Aortogastric fistula
View Answer
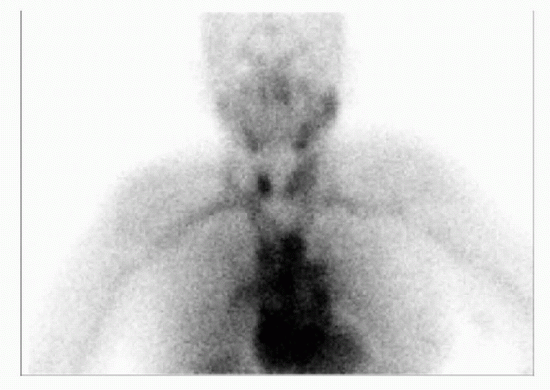
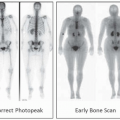
9 Answer D. The supplied images demonstrate persistent diffuse radiotracer uptake in the stomach, which does not move. The blood pool activity is markedly reduced. Activity is also seen in the renal collecting system and bladder (more so than usual). The findings are consistent with free pertechnetate. Gastric mucosal, salivary gland, thyroid gland, and renal activities are seen when free Tc-99m pertechnetate is present. When free Tc-99m pertechnetate is suspected, image of the thyroid and salivary glands should be obtained to confirm that it is the source of this artifact (see below). Of the methods for labeling autologous RBCs, in vivo technique has the worst labeling efficiency (˜75%) and higher chances of free pertechnetate. This can be avoided by using in vitro RBC-labeling method (labeling efficiency of 98%) and performing quality control to check for the free pertechnetate. In the event of gastric hemorrhage, significant amount of activity would transit into the small bowel on the subsequent images.
 |
Reference: Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:309, 310, 312.
10 Tc-99m-tagged red blood cell (RBC) scintigraphy enables detection of gastrointestinal bleeding at the rate of as low as:
A. 0.01 to 0.04 mL/min
B. 0.1 to 0.4 mL/min
C. 1 to 4 mL/min
D. 10 to 14 mL/min
View Answer
10 Answer B. Tc-99m-tagged RBC scintigraphy has a high sensitivity in detecting bleeding rates as low as 0.04 to 0.2 mL/min, although total volume of 2 to 3 mL is necessary for scintigraphic detection. Comparatively, angiography will locate GI bleeding sites in up to 65% of cases when bleeding occurs at a rate >1 mL/min. Also, the bleeding must be occurring during the 20 to 30 seconds of contrast injection for the angiography to localize the bleeding site. Compared to angiography, tagged RBC scintigraphy is easy to perform, requires no patient preparation, and is noninvasive. It also provides prognostic information as the patients with negative scintigraphy will rarely require urgent surgery.
References: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:247.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: The requisites, 4th ed. Philadelphia, PA: Saunders, 2014:307-314, 435.
11 If Tc-99m-labeled RBC scintigraphy cannot be performed, which other radiotracer may be used for the evaluation of gastrointestinal bleeding?
A. Tc-99m sulfur colloid
B. In-111 DTPA
C. I-123 MIBG
D. Tc-99m DMSA
View Answer
11 Answer A. Tc-99m sulfur colloid (SC) was the first radiopharmaceutical to be utilized for the evaluation of gastrointestinal bleeding (GI). An advantage of Tc-99m SC is rapid clearance from the intravascular space by the reticuloendothelial system (half time 2 to 3 minutes); this permits clear visualization of the extravasated radiotracer from the bleeding site. This is also a disadvantage as limited intravascular residence time (<10 minutes) increases the chance of missing an intermittent bleed. Also, prominent liver and spleen activity may obscure the bleeding sites in parts of the transverse colon, stomach, and duodenum. In contrast, Tc-99m RBCs remain within the intravascular space and can usually be imaged up to 24 hours after the injection, allowing for the detection of the intermittent GI bleed. As such, Tc-99m RBCs are the radiopharmaceutical of choice for performing the GI bleeding scintigraphy.
References: Dam HQ, Brandon DC, Grantham VV, et al. The SNMMI procedure standard/EANM practice guideline for gastrointestinal bleeding scintigraphy 2.0. J Nucl Med Technol 2014;42(4):308-317.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:307-314, 308.
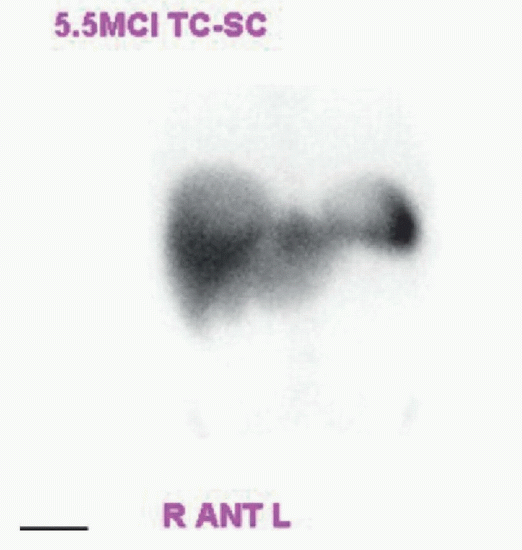
12 The image below is that of a liver-spleen scan. How long after the intravenous administration of Tc-99m sulfur colloid is the imaging usually initiated?
 |
A. 10 minutes
B. 20 minutes
C. 40 minutes
D. 60 minutes
View Answer
12 Answer B. Approximately 2 to 6 mCi of Tc-99m sulfur colloid (SC) is injected intravenously for the liver spleen scintigraphy. It undergoes rapid clearance from the intravascular space by the reticuloendothelial system with the intravascular half time of about 2 to 3 minutes. Majority (>98.4%) of the radiopharmaceutical would be removed from the intravascular blood pool in six half-lives (18 minutes). As such, imaging is usually commenced 20 minutes after the IV injection of Tc-99m SC.
Reference: Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:307-314, 161-164.
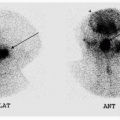
13 The following image is from a 62-year-old lady who underwent splenectomy for idiopathic thrombocytopenic purpura (ITP) approximately 10 years ago. What is the most likely diagnosis?
 |
A. Focal nodular hyperplasia
B. Accessory spleen
C. Common bile duct obstruction
D. Acute cholecystitis
E. Intra-abdominal abscess
F. Lymphoma
View Answer
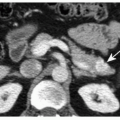
13 Answer B. A small focus of intense uptake is seen in the left upper quadrant on the posterior image of this heat-damaged Tc-99m-tagged red blood cell (RBC) scan. This is consistent with an accessory spleen or residual splenic tissue. Removal of abnormal erythrocytes by the reticuloendothelial system is the basis for denatured RBC uptake by the functioning splenic tissue. In this study, the Tc-99m-labeled RBCs are heat damaged for 20 minutes in a water bath at 49°C to 50°C. This causes them to become rigid spherocytes that upon reinjection are phagocytosed by the reticuloendothelial system. Normal physiologic distribution of denatured RBCs is in the liver, spleen, and bone marrow. In cases of ITP, recurrence after splenectomy prompts evaluation of residual splenic tissue. This exam can also be used in the diagnosis of splenosis after trauma (arrows in the image below).
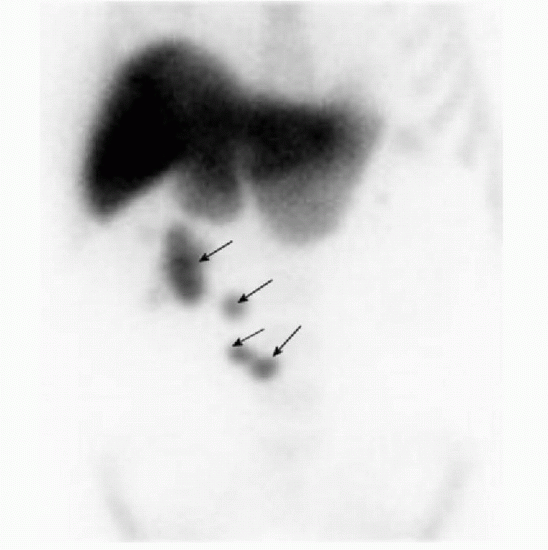 |
Reference: Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:307-314, 163-164.
14 A patient presents for the evaluation of residual splenic tissue after splenectomy. In which of the following instances, the heat damaged red blood scan is preferred over the Tc-99m sulfur colloid scintigraphy?
A. Lesion is adjacent to the liver.
B. Lesion is in the chest.
C. Lesion is adjacent to the bladder.
D. Lesion is in the splenic hilum.
E. Lesion is in the mesentery.
View Answer
14 Answer A. The Tc-99m sulfur colloid (SC) is taken up by the reticuloendothelial system and is commonly used for the evaluation of residual splenic tissue. Only 5% to 10% of the injected SC localizes in the normal spleen; 80% to 90% is sequestered by the liver and <5% localizes in the bone marrow. This high liver uptake makes evaluation of the splenic tissue adjacent to the liver parenchyma difficult. Heat-damaged Tc-99m-labeled red blood cell (RBC) scan is more sensitive for the evaluation of residual splenic tissue as the denatured RBCs are sequestered by the splenic tissue in high concentration. This is due to their larger size compared to the SC. Relatively higher uptake of denatured RBCs by the splenic tissue compared to the liver allows for a better differentiation of a splenule from the adjacent liver parenchyma.
Reference: Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:307-314, 163-164.
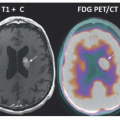
15 The following arterial phase CT as well as anterior and posterior planar images are from a patient with a mass within the lateral segment of the left hepatic lobe. What is the most likely diagnosis?
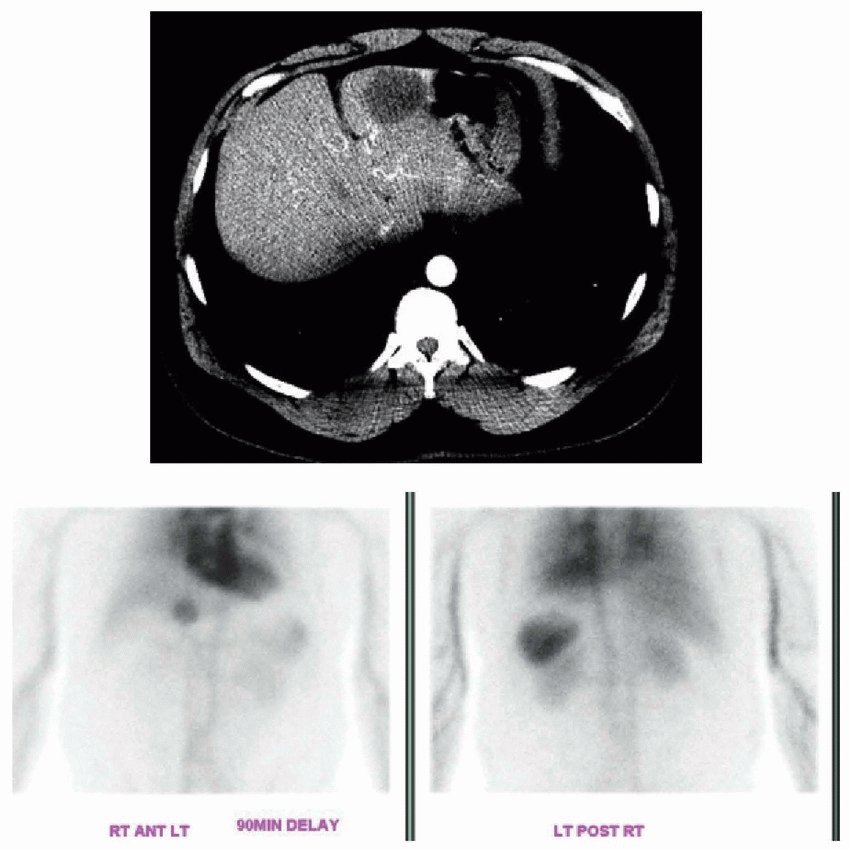 |
A. Focal nodular hyperplasia
B. Hepatocellular carcinoma
C. Cavernous hemangioma
D. Solitary metastasis
E. Hepatic adenoma
F. Hepatic abscess
View Answer
15 Answer C. The anterior and posterior projection images from a 90-minute delayed Tc-99m RBC scan demonstrate intense physiologic activity in the blood pool and spleen with mild-to-moderate physiologic activity in the liver and kidneys. A moderate-sized focus of intense uptake in the lateral segment of the left hepatic lobe (arrow in the anterior image below) is consistent with a hemangioma. On Tc-99m RBC scan, hemangioma generally has decreased intensity compared to adjacent liver on early flow images and increased intensity compared to adjacent liver on the 90- to 120-minute delayed images. Radiotracer uptake of hemangioma is often equal to that of blood pool, but heterogeneous uptake can be seen with giant cavernous hemangioma. Tc-99m RBC scintigraphy has near 100% positive predictive value for diagnosing hemangioma. Other lesions present as areas of reduced tracer uptake (“cold”) on the tagged RBC scans.
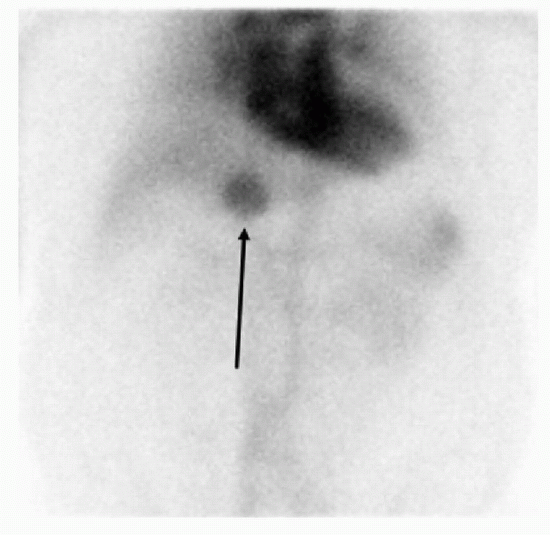 |
Reference: Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:307-314, 156-160.
16 What is the most common cause of a false-negative Tc-99m RBC scintigraphy for a hemangioma?
A. Poor injection bolus
B. Peripheral location of the lesion
C. Central location of the lesion
D. Small size of the lesion
View Answer




16 Answer D. The most common cause of a false-negative Tc-99m RBC scintigraphy for hemangioma is its small size. Performing SPECT significantly improves the sensitivity of tagged RBC scan for hemangioma detection when compared to the planar imaging, especially if the lesions measure <2.5 to 3.0 cm. The SPECT imaging using Tc-99m RBCs has close to 100% sensitivity for lesions >1.5 cm in diameter, which decreases to <50% for lesions <1 cm. Other reported causes of false-negative study include the hemangioma being adjacent to a vascular structure (such as the heart, portal vein, or IVC), extensive fibrosis within the hemangioma, and perceived increased activity on the flow images.
Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
