Genitourinary System
QUESTIONS
1 What percent of renal plasma flow is usually cleared by the glomerular filtration?
A. 10%
B. 20%
C. 40%
D. 80%
View Answer
1 Answer B. Twenty percent of renal plasma flow is cleared by the glomerular filtration, and 80% is cleared by the tubular secretion.
Reference: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:315.
2 A 35-year-old potential renal transplant donor presents for the evaluation of glomerular filtration rate (GFR) as a part of preoperative workup. Which of the following radiopharmaceuticals would be most appropriate to use in this situation?
A. MAG3
B. DTPA
C. DMSA
D. Glucoheptonate
View Answer
2 Answer B. Diethylenetriamine pentaacetic acid (DTPA) is filtered through the glomeruli and can therefore be used to estimate the GFR. Approximately 5% to 10% of the radiopharmaceutical is bound to plasma protein resulting in a slight underestimation of the GFR. Mercaptoacetyltriglycine (MAG3) is cleared predominantly via proximal tubular secretion with minimal filtration. Higher extraction efficiency and plasma protein binding of MAG3 make it a better agent for evaluation of renal flow and function, but it cannot measure the GFR. Dimercaptosuccinic acid (DMSA) is a renal cortical imaging agent, which is primarily used in the pediatric population for evaluation of pyelonephritis, renal cortical scarring, and differential renal function. Glucoheptonate is cleared via both glomerular filtration and renal tubule secretion and cannot be used to calculate the GFR as well. The measured GFR is used as a confirmatory test for the estimated GFR in certain clinical situations such as severe malnutrition or obesity, diseases of skeletal muscle, or in the evaluation of donor renal function prior to transplantation.
References: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:315-316.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:170-175.
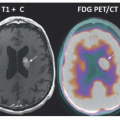
3 A 36-year-old lady with extensive past medical history including multiple prior cancers presents for restaging on FDG-PET/CT. Based on the following images, what is the most likely diagnosis?
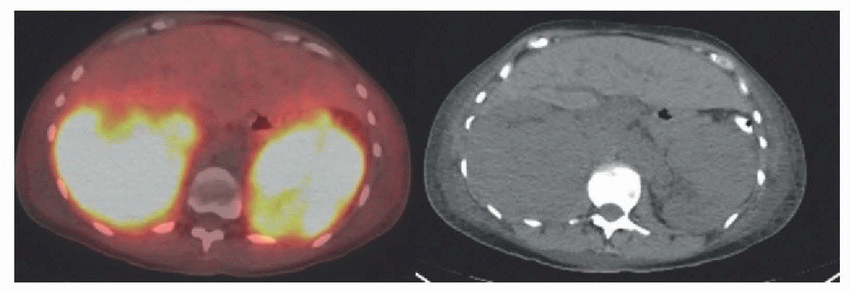 |
A. Hydronephrosis
B. Bilateral urine leak
C. Acute tubular necrosis
D. Lymphoma
E. Renal cell carcinoma
View Answer
3 Answer D. Images demonstrate intense parenchymal uptake in enlarged kidneys bilaterally. This is classic for renal lymphoma. Renal lymphoma can also present with multiple hypermetabolic masses or hypermetabolic soft tissue surrounding the kidneys. There is no dilatation of the collecting system to suggest obstruction or hydronephrosis. ATN would not present with enlarged kidneys. Renal cell carcinoma would be more likely to present with focal unilateral involvement and typically demonstrate lower degree FDG uptake on the PET images than what is seen.
Reference: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:381-390.
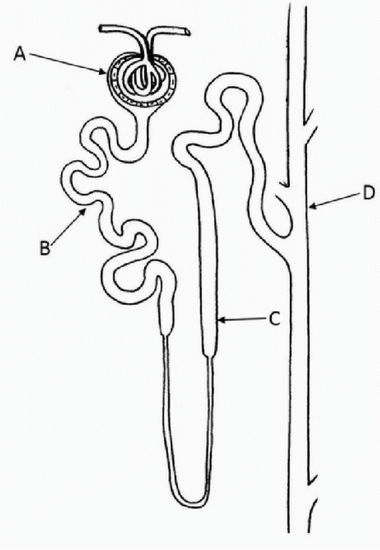
4 In the following diagram of the renal nephron, where does DMSA localize on the 2- to 4-hour images acquired for the renal cortical imaging?
 |
View Answer
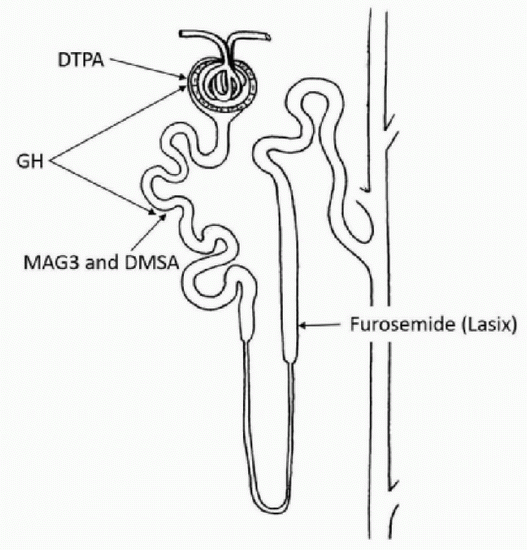
4 Answer B. DMSA is a renal cortical imaging agent that localizes in the renal cortex by binding to the sulfhydryl groups in the proximal renal tubules. Glomerular filtration of DMSA followed by tubular reabsorption is the predominant route of DMSA uptake by the kidney. MAG3 is primarily removed from the plasma by active transport in the proximal renal tubules (Choice B). DTPA is filtered through the glomerulus (Choice A). Tc-99m glucoheptonate (GH) is both filtered by the glomerulus and secreted by the renal tubules, allowing for evaluation of renal function and collecting system. Approximately 10% to 15% of the injected GH dose remains bound to the renal tubules at 1 to 2 hours after the injection, and thus, it can also be used for renal cortical imaging. Loop diuretics (i.e., furosemide and bumetanide) block the Na+/K+/2Cl− cotransporter that is present in the loop of Henle. The following diagram shows the location of the localization of different radiopharmaceuticals in the renal nephron.
 |
References: Taylor AT. Radionuclides in nephrourology, part 1: radiopharmaceuticals, quality control, and quantitative indices. J Nucl Med 2014;55(4):608-615.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:170-175.
5 The following patient presents for the evaluation of renal function and possible obstruction. Renal scintigraphy using which of the following radiopharmaceutical is MOST appropriate in this situation?
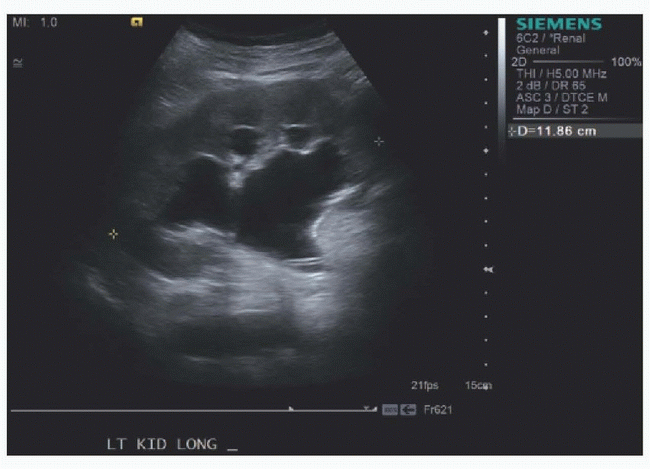 |
A. DTPA
B. MAG3
C. DMSA
D. Hippuran
View Answer
5 Answer B. The renal sonogram demonstrates moderate to severe hydronephrosis. In the setting of obstruction, GFR typically declines before tubular secretion. Additionally, the extraction fraction of MAG3 is 40% to 50%, more than twice that of DTPA. As such, MAG3 is preferred over DTPA in patients with suspected obstruction and impaired renal function. MAG3 is also the preferred radiopharmaceutical for renal function evaluation in the pediatric population because glomerular filtration is incompletely developed in the neonates. It is currently the most commonly used renal radiopharmaceutical. While DMSA would be useful in the evaluation of differential renal function, it would not allow assessment of obstruction as it remains predominately fixed in the renal tubule and not excreted into the renal collecting system. Hippuran required labeling with I-131 or I-123 and produced poor imaging quality images; it has been replaced by Tc-99m MAG3.
References: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:324-325.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:170-175.
6 Which of the following is the preferred radiopharmaceutical in the determination of the differential renal function?
A. DTPA
B. MAG3
C. DMSA
D. Glucoheptonate
E. Hippuran
View Answer
6 Answer C. DMSA is cortically bound and demonstrates very little renal excretion compared to the other renal agents. For this reason, it is the best agent to determine differential renal function. This lack of significant renal excretion is particularly useful in the setting of hydronephrosis. Differential renal function provided by Tc-99m MAG3 is also accurate in the absence of hydronephrosis. It is calculated by measuring the counts in each renal region of interests at the peak activity (1 to 3 minutes after the injection) before the radiopharmaceutical is excreted into the collecting system. When the main concern is the determination of the differential renal function, DMSA is the radiopharmaceutical of choice.
References: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:316.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:170-175.
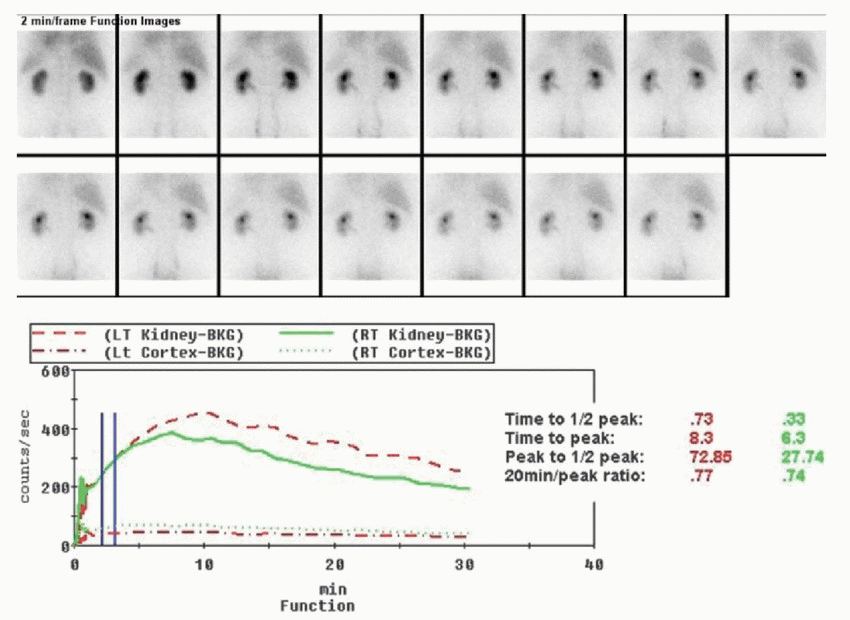
7 Based on the following renal function images and accompanying time activity curve (renogram) from a MAG3 dynamic renography, what is the most likely diagnosis?
 |
A. Normal renal function
B. Mildly impaired renal function
C. Moderately impaired renal function
D. Severely impaired renal function
E. Bilateral renal artery stenosis
F. Bilateral obstructive hydronephrosis
View Answer
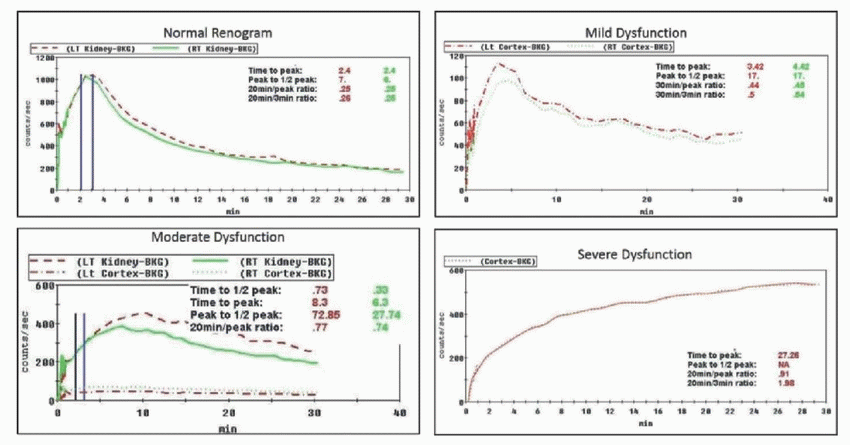
7 Answer C. Normal MAG3 time activity curve (renogram) demonstrates prompt tubular extraction (time to peak 3 to 5 minutes) with good renal clearance/excretion (time to half peak 6 to 10 minutes or 20 minutes to peak ratio of <0.3) as shown in image below. Mild renal function impairment demonstrates normal tubular extraction with normal time to peak and slightly prolonged renal clearance (slightly prolonged 20 minutes to peak ratio), which would manifest as mild retention of radiotracer in the renal parenchyma at the end of 30 minutes. With moderate renal function impairment, there is tubular dysfunction (prolonged time to peak) and moderate cortical retention (prolonged 20 minutes to peak ratio). With severe renal function impairment, there is poor uptake with progressive accumulation and no significant clearance of the radiopharmaceutical (markedly prolonged time to peak). While renal scintigraphy and renogram are good in determining the degree of renal dysfunction, the exact cause of dysfunction (i.e., ATN, pyelonephritis, drug toxicity, or chronic medical renal disease) depends on the patient’s medical history. Of note, the patient should be well hydrated for dynamic renography. While blood flow and radiopharmaceutical uptake are not altered by dehydration, excretion and washout may be delayed simulating poor function or obstruction. Renogram curves must be interpreted in conjunction with the images as they can be affected by numerous factors including hydronephrosis.
 |
References: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:317-321.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:175-179.
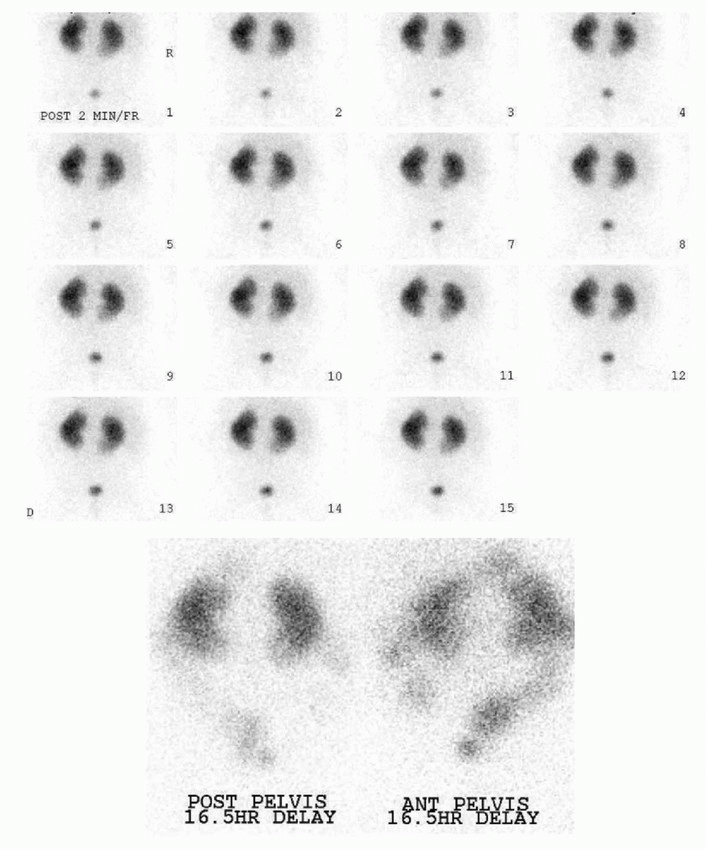
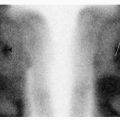
8 The following renal scintigraphy was performed on a 2-year-old with decreased urine output. What is your interpretation of the findings?
 |
A. Normal
B. Urine leak
C. Renal-colic fistula
D. Severe renal dysfunction
E. Bilateral hydronephrosis
View Answer
8 Answer D. Initial images demonstrate no significant radiotracer excretion; therefore, delayed images were acquired. On delayed images, there is persistent renal activity at 16.5 hours compatible with severe renal dysfunction. Activity is also noted within bowel. The alternative path of the technetium-99m MAG3 excretion is by the hepatobiliary system. So, bowel activity may be visualized on the delayed images in patients with severely diminished renal function. A renal-colic fistula typically develops after a procedure such as renal ablation, and if this was the case, activity should have been present in the bowel on the initial images.
Reference: Shea TE, Pfister RC. Opacification of the gallbladder by urographic contrast media reflection of an alternate excretory pathway. Am J Roentgenol Radium Ther Nucl Med 1969;107(4):763-768.
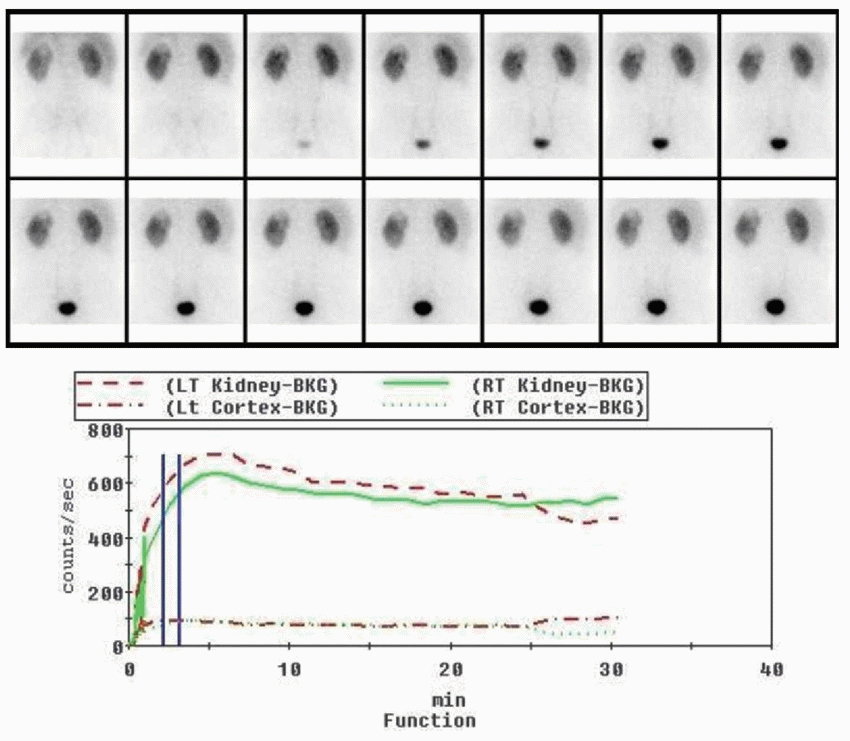
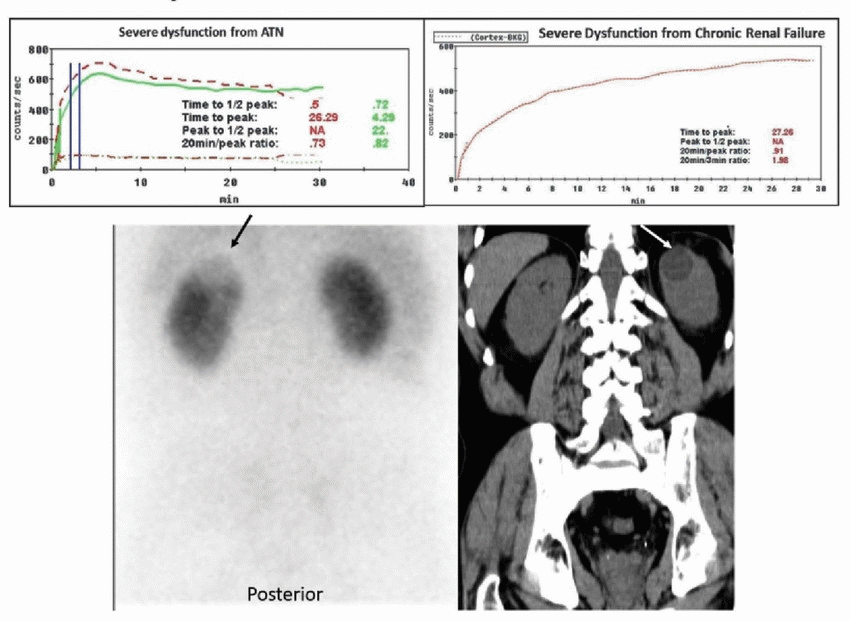
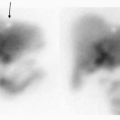
9 The following Tc-99m MAG3 functional renal scintigraphy images as well as time activity curves are from a 60-year-old who was admitted with dehydration and elevated creatine kinase levels. What is the most likely diagnosis?
 |
A. Acute tubular necrosis
B. Severe chronic renal disease
C. Bilateral hydronephrosis
D. Bilateral renal artery stenosis
View Answer
9 Answer A. Dynamic posterior images acquired after the IV administration of MAG3 demonstrate brisk uptake of the radiopharmaceutical within both kidneys. However, there is minimal excretion. Findings are most compatible with acute tubular necrosis in this patient with dehydration and rhabdomyolysis. In severe chronic renal disease, due to chronic tubular dysfunction, the rate of radiopharmaceutical concentration would be lower with gradual upslope instead of brisk upstroke (see renograms below). There is no evidence of dilated renal collecting system on the supplied images to suggest hydronephrosis. Since captopril was not given for the examination, renal artery stenosis is not a possibility. Of note, a small area of photopenia within the upper pole of the left kidney (arrow) corresponded to a renal cyst. Since the peak uptake in normal kidney occurs between two and five minutes, nonfunctioning renal tissue or photopenic defects (i.e., cyst, renal cell carcinoma, or metastasis) are be best appreciated during this time period.
 |
References: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:317-321.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:175-179.
10 In the setting of renal artery stenosis, how does the renin-angiotensin axis maintain the glomerular filtration rate (GFR)?
A. Afferent arteriolar vasoconstriction
B. Afferent arteriolar vasodilatation
C. Efferent arteriolar vasoconstriction
D. Efferent arteriolar vasodilatation
E. Diffuse dilation throughout the capillary bed
F. Diffuse constriction throughout the capillary bed
View Answer
10 Answer C. In the setting of renal artery stenosis, the juxtaglomerular apparatus of the kidneys produces renin, which converts angiotensinogen to angiotensin I in the liver. Angiotensin I gets converted to angiotensin II by the angiotensin-converting enzyme (ACE) in the lung parenchyma. One of the actions of angiotensin II is efferent arteriolar constriction. This increases the net gradient pressure across the glomerulus and helps maintain the GFR. ACE inhibitors block the conversion of angiotensin I to angiotensin II in the lung parenchyma. The resultant inhibition of efferent arterial constriction causes decrease in the GFR with resultant renal function impairment.
References: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:328-336.
Saha GB. Fundamentals of nuclear pharmacy, 6th ed. New York, NY: Springer, 2010:296.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:184-188.
11 What is the most appropriate management in this patient with the following renal scintigraphy findings?
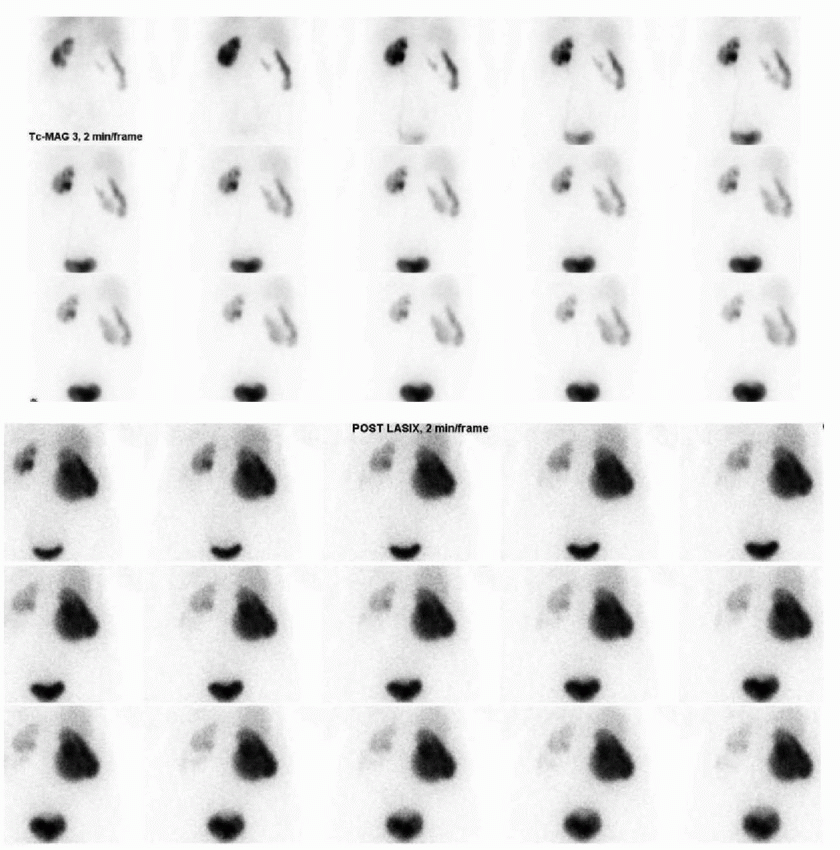 |
A. Nephrectomy
B. Pyeloplasty
C. Ureteral reimplantation
D. Cystectomy
E. Ileal conduit
View Answer
11 Answer B. Posterior dynamic MAG3 renal scintigraphy images demonstrate enlarged right kidney with a large central area of photopenia, which fills in with the radiotracer on the delayed images. There is no significant emptying of this tracer after administration of Lasix. Findings represent hydronephrosis with right ureteropelvic junction (UPJ) obstruction. The left kidney appears normal. Pyeloplasty is typically the initial management in patients with UPJ obstruction. If corrected promptly, renal function can recover fully. Nephrectomy is reserved for cases with minimal residual renal function; in this case, the function may be mildly impaired. Ureteral reimplantation, cystectomy, and ileal conduit would not help in the management of a UPJ obstruction.
Diuretic renography can help distinguish obstructive from nonobstructive hydronephrosis. Increase in the urine flow caused by Lasix administration in a dilated but nonobstructed system would lead to washout of the accumulated radiopharmaceutical. In obstructive hydronephrosis, there would be progressive filling of the dilated collecting system, which does not empty after Lasix administration. This can be quantified using time-activity curve by measuring the amount of time it takes to reach half the level of the activity, known as the diuretic T1/2 time. Diuretic T1/2 time of <10 minutes suggests nonobstructive hydronephrosis, while that >20 minute suggests obstructive hydronephrosis. Diuretic T1/2 time of 10 to 20 minutes is indeterminate for obstruction.
References: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:324-329.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:179-184.
12 Based on the provided pre- and post-Lasix images and the Lasix renogram curve, what is the most likely diagnosis?
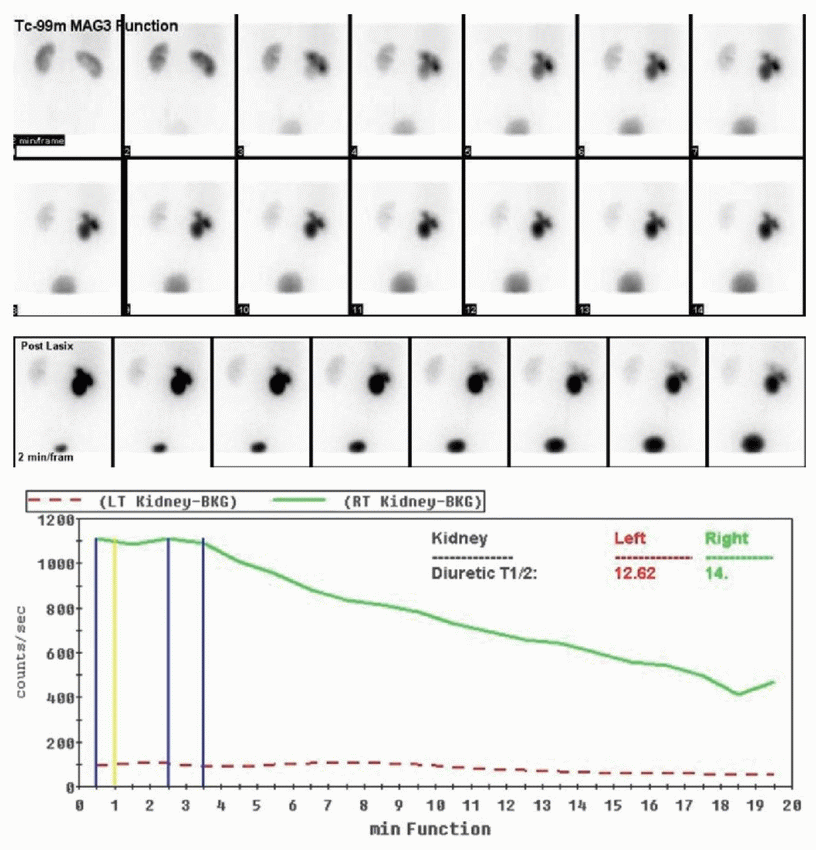 |
A. Right hydronephrosis with obstruction
B. Right hydronephrosis without obstruction
C. Right hydronephrosis indeterminate for obstruction
D. Poorly functioning right kidney
E. Poorly functioning left kidney
F. Left hydronephrosis with obstruction
G. Left hydronephrosis without obstruction
H. Left hydronephrosis indeterminate for obstruction
View Answer
12 Answer C. Posterior dynamic Tc-99m MAG3 functional images demonstrate a central area of photopenia in the right kidney from pelvicaliectasis with abnormal rotation on the functional images. Brisk uptake and excretion indicate good bilateral renal function. There is progressive accumulation of radiopharmaceutical in the right pelvicalyceal system indicating marked right hydronephrosis. After Lasix administration, there is some emptying of the radiopharmaceutical from the hydronephrotic right collecting system with the indeterminate diuretic T1/2 emptying time of 14 minutes. This slow partial clearance may be a result of an extremely distended system with large capacitance, and an obstruction may not be present; however, since obstruction cannot be entirely excluded, Lasix T1/2 time values between 10 and 20 minutes obstruction are assigned an indeterminate for obstruction category. In addition to increased capacitance, indeterminate Lasix T one-half emptying time can also be caused by dehydration and poor diuretic response in a patient with severe chronic kidney disease.
References: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:324-329.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:179-184.
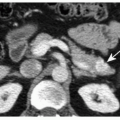
13 A 45-year-old lady with HTN and back pain was found to have an abnormality on a recent contrast-enhanced CT scan. Based on the supplied images, which of the following is the most likely diagnosis?
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


