Germ cell tumors (GCTs) are a heterogeneous group of central nervous system (CNS) tumors with morphologic, immunophenotypic, and genetic homologs of gonadal and other extra-CNS germ cell neoplasm but with distinct clinical behavior and possibly in their cellular origin. There are six main histologic variants of CNS GCTs: germinoma, teratoma, yolk sac tumor, embryonal carcinoma, choriocarcinoma, and mixed cell type. CNS GCTs likely develop through combined genetic and epigenetic mechanisms from a common ancestral cell and share identical somatic mutations in the MAPK/PI3K pathway. GCTs are one of the more common solid tumors of childhood and occur more frequently in young adolescent males living in Japan and other Asian countries than in North America and Europe.
Age range (mean)
Female: male ratio
Cell of origin
Serum/CSF tumor markers
Molecular/genetic markers
Prognosis
Germinoma
7-30 (19.2)
Overwhelming gender majority is males, with ratio of 1:15
Somatic tissues derived from germ layers (ectoderm, endoderm, mesoderm)
–
–
Intermediate
Mixed germ cell tumor
0-20 (14)
Several germ cell components
Yolk sac tumor
8-23
Primitive germ cell
AFP
AFP
Poor
Embryonal carcinoma
8-23
Large epithelioid cells of embryonic germ disc
–
CD30
CK AE1/3
Poor
Choriocarcinoma
8-23
Non-germinomatous malignant germ cell
HCG
HCG
Poor
AFP, alpha-fetoprotein; ASK, arabidopsis skp-like; CD, cluster of differentiation; CK, cytokeratin, pan antibody; CSF, cerebrospinal fluid; HCG, human chorionic gonadotropin; KIT, KIT proto-oncogene, receptor tyrosine kinase; PLAP, placental-like alkaline phosphatase; RAS, rat sarcoma; TOR, target of rapamycin.
Germ Cell Tumors of the Central Nervous System
Definition: Germ cell tumors (GCTs) of the central nervous system (CNS) are a heterogeneous group of neoplasms with the morphologic, immunophenotypic, and genetic homologs of gonadal and other extraneuraxial GCTs. However, CNS GCTs differ from their gonadal and extraneuraxial GCTs in many aspects, including morphology, clinical behavior, and possibly their cell of origin. CNS GCTs are broadly classified as germinomatous and non-germinomatous GCTs on the basis of clinicopathological and laboratory findings and serum and CSF tumor markers.
Epidemiology: GCTs primarily affect children and adolescents, male more frequently than female, with much higher geographic prevalence in eastern Asia (e.g., Japan, Taiwan, China, Korea) than in Europe or the United States. GCTs represent up to 15% of all pediatric brain tumors in these regions. Pure germinomas outnumber other histologic subtypes and comprise about 40% of all GCTs.
Affected age group: Bimodal distribution of CNS GCT incidence shows a small peak for infants less than 2 years of age and a larger peak for adolescents (13-19 years). The vast majority of patients with GCT are younger than 25 years of age, with peak incidence coinciding with the onset of puberty. Males are more frequently affected than females, except for infantile GCT, which is more common in females. There is a large gender difference in GCTs arising in the pineal region and diagnosed in the age group of 10-19 years, where the male-to-female ratio can be higher than 9:1. It remains speculative as to why there is such great male gender predominance in GCTs in the pineal region and the young adolescent age group, but the physiological and hormonal changes in male puberty appear to favor neoplastic transformation in the male pineal region and during the height of pubescent growth. Patients with teratoma or choriocarcinoma tend to present with symptoms when they are about 10 years younger, while pure germinomas are more commonly seen in older age group, usually in the second decade. Choriocarcinomas are the rarest, most malignant CNS GCTs with elevated serum and CSF b-HCG levels.
Molecular and genetic profile: Each histologic subtype of GCT has its own unique molecular and genetic alteration.
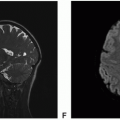
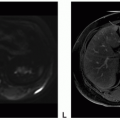
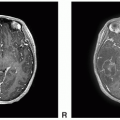
Clinical features and standard therapy: The most common location of central nervous system (CNS) GCTs is the pineal region (45%), and the second most common location is the suprasellar region (30%). Basal ganglia location is rare but well described in published reports. The signs and symptoms of CNS GCTs depend on the location of the tumor. Patients with pineal region GCTs often present with signs and symptoms of raised intracranial pressure, diplopia, and hydrocephalus related to compression of tectum and cerebral aqueduct, respectively. Patients with suprasellar region GCTs often present with hormonal deficiencies, most commonly diabetes insipidus caused by antidiuretic hormone deficiency, and chronic protracted prodrome lasting months to years.
Only gold members can continue reading. Log In or Register to continue