KEY FACTS
Terminology
- •
Autoimmune disorder with long-acting, thyroid-stimulating antibodies producing hyperplasia and hypertrophy of thyroid
Imaging
- •
Mild/moderate diffuse, symmetric enlargement of thyroid gland, including isthmus
- •
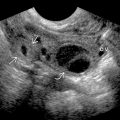
Hypoechoic, heterogeneous, spotty parenchymal echo pattern
- •
Marked increase in parenchymal vascularity (turbulent flow with AV shunts): “Thyroid inferno”
- •
Increased vascularity does not correlate with thyroid function but reflects inflammatory activity
- •
Spectral Doppler: Increase in peak flow velocity (≤ 120 cm/s) as measured in inferior thyroid artery
- •
↑ vascularity tends to ↓ in response to treatment
- •
Diagnosis based on clinical signs and symptoms and laboratory findings, ultrasound is not needed
Top Differential Diagnoses
- •
Hashimoto thyroiditis
- •
de Quervain thyroiditis
- •
Nodular goiter
Clinical Issues
- •
3rd-4th decade; M:F = 1:7
- •
Palpitations, loss of weight despite increased appetite, sweating, and wet palms
- •
Hyperdynamic circulatory state, muscle weakness, fatigue
- •
Thyroid-associated ophthalmopathy: Periorbital edema, lid retraction, ophthalmoplegia, proptosis, malignant exophthalmos
- •
Elevated T₃ + T₄ levels and depressed TSH level
- •
Strong family history of autoimmune disorders
Scanning Tips
- •
US may be used to establish thyroid volume prior to radioactive iodine treatment
 in a patient with Graves disease (GD). Diagnosis of GD is based on clinical features and laboratory tests. Ultrasound is usually not indicated for patient management.
in a patient with Graves disease (GD). Diagnosis of GD is based on clinical features and laboratory tests. Ultrasound is usually not indicated for patient management.
 . This appearance overlaps with Hashimoto thyroiditis, but the clinical picture is different.
. This appearance overlaps with Hashimoto thyroiditis, but the clinical picture is different.Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


