Histiocytic Tumors
Overview
Histiocytic tumors are a rare heterogeneous group of tumor of the hematopoietic and lymphoid tissues and broadly classified into two categories: Langerhans cell histiocytosis and non-Langerhans histiocytosis.
Tumor Subtypes
▶ Langerhans Cell Histiocytosis
▶ Erdheim-Chester Disease
▶ Rosai-Dorfman Disease
▶ Histiocytic Sarcoma
|
Langerhans Cell Histiocytosis
Definition: An immune-mediated disorder characterized by a clonal proliferation of immature Langerhans cells resulting in formation of granulomas throughout the body, especially in the skin, lymph nodes, lungs, liver, bone marrow, and brain and spine.
Epidemiology: Mostly affects children, with an annual incidence of 0.5 cases per 100,000 individuals aged <15 years, with a mean age of 1.5 years.
Molecular and genetic profile: A clonal proliferation of Langerhans cell histiocytes expresses CD1a, langerin (CD207), and S100 protein. BRAF 600E mutations seen in up to half of all cases; in BRAF-wildtype, up to half can harbor MAP2K1 mutations.
Clinical features and standard therapy: Clinical presentation depends on which part of the central nervous system (CNS) is involved but two of the most common signs and symptoms of Langerhans cell histiocytosis (LCH) are diabetes insipidus and hypothalamic dysfunction due to frequent involvement of the pituitary infundibulum and hypothalamus. Asymptomatic lytic skull lesions are not uncommon, as is complete marrow replacement of spine leading to vertebra plana.
Imaging
The imaging hallmark of LCH is proliferation and accumulation of Langerhans histiocytes primarily within the bone but also in the brain, both in the intraaxial and extra-axial compartments. Computed tomography is better suited for characterization of lytic or expansile osseous lesion and assessment of cortical breakthrough. Magnetic resonance is superior in assessment of extent of marrow involvement, soft tissue component, dural or brain invasion, and unsuspected additional lesions.
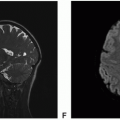
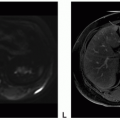
 Figure 5.1. Imaging of Langerhans cell histiocytosis of pituitary infundibulum and temporal bone. A. Coronal T1-precontrast: Soft tissue pituitary infundibular mass isointense signal to the neighboring optic chiasm. B. Sagittal T1-precontrast: Soft tissue pituitary infundibular mass isointense signal to the neighboring optic chiasm. C. Coronal T2-FSE: Soft tissue pituitary infundibular mass isointense signal to the white matter of the brain. D. Coronal T1-postcontrast: Avid enhancement of the soft tissue pituitary infundibular mass. E. Sagittal T1-postcontrast: Avid enhancement of the soft tissue pituitary infundibular mass. F. Axial CT: Lytic destructive lesion centered in the left mastoid temporal bone. |
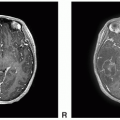
 Figure 5.1. (continued) G. Axial T1-precontrast: Mass isointense to the brain within the left mastoid temporal bone. H. Axial T2 FSE: Heterogeneous signal of the mass filling the left mastoid temporal bone. I. Coronal T1-precontrast: Mass isointense to the brain within the left mastoid temporal bone. J. Coronal T1-postcontrast. K. Sagittal T1-postcontrast. L. Axial T1-postcontrast. |
 Figure 5.2. Imaging of spinal LCH. A. Sagittal T2: Hyperintense signal replacing the marrow of collapsed C3 vertebral body. B. Sagittal T1-precontrast: Hypointense signal replacing the marrow of collapsed C3 vertebral body. C. Sagittal T1-postcontrast: Avid but heterogeneous enhancement of C3. D. Sagittal T2: Vertebra plana of L1. E. Sagittal T1-precontrast: Complete collapse of anterior half of L1 vertebral body. F. Sagittal T1-postcontrast: No enhancement within the collapsed L1 vertebral body.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|