Abstract
Vertebral osteophytes are the result of intervertebral disc degeneration and can occasionally damage the aorta located in their proximity. This paper describes the case of a 69-year-old woman with a pseudoaneurysm of the descending thoracic aorta caused by a progressively growing dorsal osteophyte. The patient was asymptomatic as the pseudoaneurysm was an incidental finding diagnosed with an 18 F-FDG PET/CT and computed tomography angiography (CTA) performed during follow-up for breast cancer. The comparison between the latest 18 F-FDG PET/CTA performed and previous exams was crucial for the diagnosis. In fact, the authors were able to demonstrate the progressive growth of the osteophyte and the subsequent development of the pseudoaneurysm. Both morphological features and metabolic behaviors supported the diagnosis. The pseudoaneurysm was successfully treated with thoracic endograft.
Introduction
Aortic injuries may occur after a blunt or penetrating trauma. A few cases of aortic injuries induced by osteophytes following acute trauma have been described [ ]. In older patients, disc degeneration leads to osteoarthritis, which is often associated with osteophyte growth on vertebral bodies. Osteophytes’ growth commonly occurs between the T4 and T10 vertebrae and few studies show that increase in age is a predisposing factor [ ]. Two types of osteophytes can form on the anterior aspects of the vertebrae: claw, traction and fusion types. In particular, the claw type can sometimes form a sharp edge [ ]. With age, large arteries’ walls are less flexible and more susceptible to erosive action of osteophytes. The stress occurring from osteophytes may render the overlying aortic wall ischemic and thus more vulnerable to infection or perforation [ ]. Aortic injuries caused by a vertebral osteophyte without major trauma have not previously been described. We report a case of pseudoaneurysm of the thoracic aorta caused by dorsal osteophyte detected with 18 F-fluorodeoxyglucose positron emission tomography/computed tomography angiography ( 18 F-FDG PET/CTA). The patient was not symptomatic and did not recall any kind of physical trauma. To confirm the relationship between the pseudoaneurysm and the osteophyte, we demonstrated first the appearance, then the progressive growth of the osteophyte and finally the development of the pseudoaneurysm by re-evaluating the previous 18 F-FDG PET/CTA scans performed during patient’s oncological follow-up.
Case report
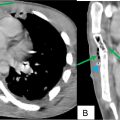
A 69-year-old woman performed 18 F-FDG PET/CTA scan as her regular follow-up for breast cancer. She underwent right mastectomy 5 years before, for infiltrating ductal breast carcinoma (pT2pN1M0 Stage IIb, G3) and has been on therapy with ribociclib and fulvestrant. She was asymptomatic, with no previous cardiovascular events, nondiabetic. She also reported hypertension under treatment. The patient did not report any physical trauma. The 18 F-FDG PET/CTA scan revealed a focal uptake (maximum standardized uptake value (SUVmax) 5.6) at the postero-medial wall of the descending thoracic aorta, located at T5-T6 level, in close proximity to a claw spinal osteophyte. The osteophyte took contact with the vessel wall ( Figs. 1 A and B), and at the same level the CTA scan showed an aortic pseudoaneurysm ( Figs. 1 C and D). Six months earlier, the 18 F-FDG PET/CTA scan revealed a bony spur at the T5-T6 level with lower tracer uptake (SUVmax 4.7) without significative atheroma or pseudoaneurysm at the level of the descending thoracic aorta ( Fig. 2 ). The revision of previous CT scans proved first the absence, then the progressive growth and modification of osteophyte density and shape ( Fig. 3 ). Based on the radiological and metabolic features and considering the development of the pseudoaneurysm in only 6 months, the Interventional Vascular Radiologist decided to treat the aortic pseudoaneurysm with the placement of a custom-made endoprosthesis ( Fig. 4 ). The postoperative course was uneventful, and the patient left the hospital the day after the procedure.

Related posts:
 Breast cancer with medullary features shows a fast and plateau enhancement pattern on magnetic resonance images: A case report
Breast cancer with medullary features shows a fast and plateau enhancement pattern on magnetic resonance images: A case report
 A rare and life-threatening case of spontaneous hemopneumothorax presenting with severe hemodynamic instability
A rare and life-threatening case of spontaneous hemopneumothorax presenting with severe hemodynamic instability
 Postextubation negative-pressure pulmonary edema after an appendectomy
Postextubation negative-pressure pulmonary edema after an appendectomy
 Primary sternal osteomyelitis in an immunocompetent adolescent
Primary sternal osteomyelitis in an immunocompetent adolescent
 Avascular necrosis of lateral femoral condyle in a middle-aged woman from central India
Avascular necrosis of lateral femoral condyle in a middle-aged woman from central India
 Facial nerve palsy from temporal bone metastasis in papillary carcinoma of thyroid: A case report
Facial nerve palsy from temporal bone metastasis in papillary carcinoma of thyroid: A case report
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


