Clinical history is essential in establishing an accurate diagnosis.
Important information includes answering these questions:
Is there a history of a previous lesion or underlying malignancy?
Is the lesion painful, or did the patient note a painless mass?
Is there a history of notable trauma or anticoagulants?
Has the lesion remained stable over a long period of time, varied in size, or is it growing?
Is there more than one lesion?
on tumor invasion into the deep dermis or through the dermis into the subcutaneous fat), and may be the only radiologic manifestation of metastases (17). Finally, multiple myxomas may be seen in association with fibrous dysplasia of bone (Mazabraud syndrome) (18). These myxomas are usually intramuscular and the association is most frequent with polyostotic disease (18, 19).
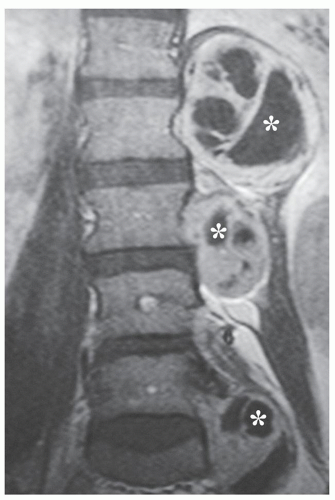 FIGURE 3.1 Neurofibromatosis: Woman, 36 years of age, presenting with multiple soft tissue masses. Coronal contrastenhanced T1-weighted (TR/TE; 500/15) spin-echo MR image shows multiple left paraspinal masses with cystic change (asterisks). |
Evaluation of a soft tissue mass must begin with radiographs.
Radiographs may be diagnostic of a palpable lesion caused by a skeletal deformity or exostosis.
Radiographs may also reveal soft tissue calcifications that can suggest a specific diagnosis.
Radiographs are the best initial method of assessing coexistent osseous involvement.
MR imaging is the preferred modality for evaluating soft tissue lesions.
Lesions should be imaged in at least two orthogonal planes.
Standard spin-echo MR pulse sequences are most useful in establishing a specific diagnosis.
Fat-suppressed fluid sensitive imaging accentuates subtle lesions by increasing lesion-to-background signal intensity.
Gradient-echo imaging is useful in demonstrating hemosiderin, metal, hemorrhage, and air.
Short-tau inversion recovery (STIR) is more sensitive for the identification of abnormal tissue.
STIR and fat-suppressed imaging reduce variations in signal intensities that are helpful in tissue characterization.
Field of view is dictated by the size and location of the lesion.
In general, a small field of view is preferred.
planes may also be a useful adjunct. In these additional planes, it is valuable to use a combination of conventional T1- and T2-weighted spin-echo images, turbo (fast) spinecho images, gradient images, and short-tau inversion recovery (STIR) images, as the case requires.
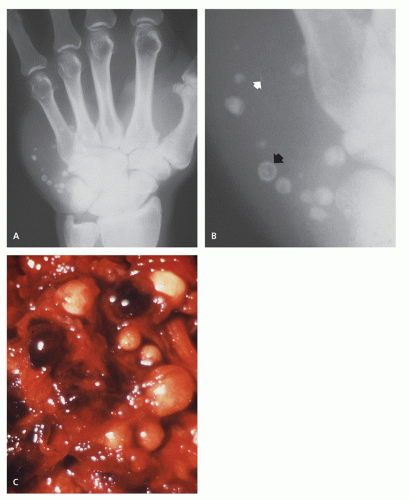 FIGURE 3.2 Phleboliths: Hemangioma in the hypothenar eminence of hand of a 52-year-old man. A: Radiograph shows hypothenar mass with multiple calcifications. B: Columnated radiograph shows multiple, small, smooth, rounded calcifications (black arrow), more opaque peripherally, characteristic of phleboliths. Note small, nonspecific calcifications (white arrow). C: Corresponding intraoperative photograph shows multiple phleboliths within interstices of hemangioma. |
with increased water content, and, as such, is useful in confirming subtle areas of soft tissue abnormality (34). This technique increases lesion conspicuity (34, 35) but typically has lower signal-to-noise than does spin-echo imaging and is also more susceptible to degradation by motion (30, 34). Lesions are generally well seen on standard imaging, and, in our opinion, STIR imaging tends to reduce the variations in signal intensities identified on conventional spin-echo MR imaging, signal intensities which are most helpful in tissue characterization.
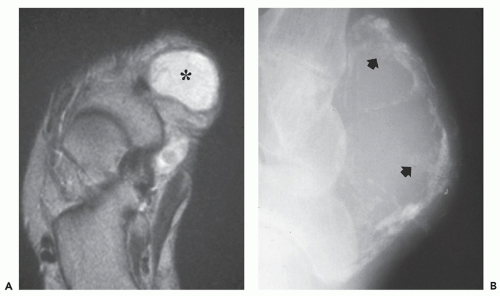 FIGURE 3.3 Synovial sarcoma: Mass in the foot of a 17-year-old girl presenting with slowly growing painless mass. A: Axial conventional T2-weighted (TR/TE; 1800/80) spin-echo MR image shows well-defined, nonspecific, soft tissue mass (asterisk). B: Corresponding radiograph shows peripheral and central calcification. The peripheral mineralization (arrows) does not show the ossification required to suggest myositis ossificans. Equally important, the history of a growing mass should also exclude this diagnosis. This radiographic appearance (calcified soft tissue mass), in context of slowly growing juxta-articular mass in a young adult, strongly suggests the appropriate diagnosis. |
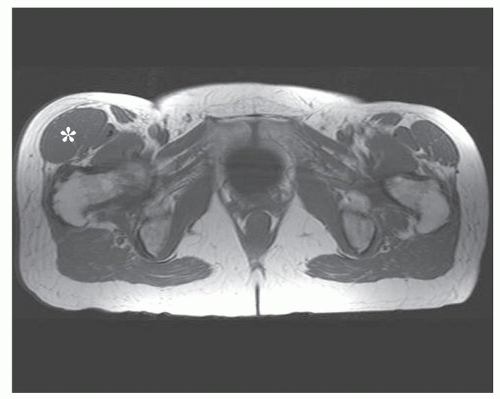 FIGURE 3.4 Hypertrophied muscle: Mass-like soft tissue asymmetry in the right thigh suggesting a mass in a 76-yearold woman. Axial T1-weighted (TR/TE; 640/15) spin-echo MR image shows the marked hypertrophy of the right tensor fascia lata muscle (asterisk), an uncommon clinical variant. |
to place a marker over the area of clinical concern, to ensure that it is appropriately imaged. This becomes important in evaluating lesions such as subcutaneous lipoma or lipomatosis, in which the lesion may not be appreciated as being distinct from the adjacent adipose tissue. When small superficial lesions are being evaluated, care should be taken to ensure that the marker or patient position does not compress the mass.
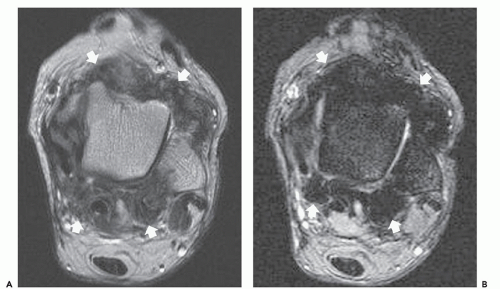 FIGURE 3.5 Hemosiderin identification with gradient-echo imaging: Pigmented villonodular synovitis (PVNS) in the ankle of a 23-year-old woman. A: Axial fast spin-echo T2-weighted (TR/TE; 4570/80) MR image shows a mass surrounding the ankle (arrows) with intermediate-to-decreased signal intensity. B: Corresponding axial gradient-echo (TR/TE; 785/20) MR image shows marked decreased signal from the mass (arrows) caused by the greater magnetic susceptibility of the hemosiderin-laden tissue, characteristic of PVNS. |
Magnetic resonance contrast agents:
Enhance the signal intensity on T1-weighted spinecho MR images of many tumors.
Enhance the demarcation between tumor and muscle and tumor and edema.
Enhance tissue vascularity and perfusion.
Malignant lesions generally show greater enhancement and greater rate of enhancement than benign lesions.
Overlap in enhancement patterns and rates between benign and malignant lesions are sufficiently great that they are of limited practical value in any specific case.
Gadolinium-enhanced imaging is useful in:
Evaluating hematomas.
Differentiating solid from cystic lesions.
Identifying cystic or necrotic areas within solid tumors.
Identifying optimal biopsy site.
 FIGURE 3.6 Field of view: Giant cell tumor of tendon sheath arising from the iliopsoas tendon in a 50-year-old woman presenting with hip pain. Columnated T1-weighted (TR/TE; 683/17) spin-echo MR image obtained with a 20-cm field of view shows the mass (asterisk) to be intimately associated with the iliopsoas tendon (arrow). This relationship was essential in suggesting the appropriate diagnosis preoperatively. |
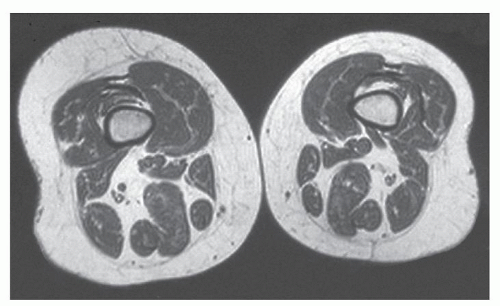 FIGURE 3.7 Contralateral extremity: Mild lipomatosis of the right lower extremity in a 54-year-old woman who presented with “fullness” around knee. Axial T1-weighted (TR/TE; 700/16) spin-echo MR image of both distal thighs shows increased adipose tissue on right as compared to contralateral side. Images of both distal thighs were obtained after no cause for clinical findings was found on axial images of right knee. |
noted in 41% of examinations; however, the majority of these were designated as mild.
A correct diagnosis is reached on the basis of imaging in about 50% of cases.
MR diagnosis is usually made on lesion signal intensity, pattern of growth, location, and associated “signs” and findings.
When a lesion has a nonspecific MR imaging appearance, a suitably ordered differential diagnosis can be formulated on the basis of tumor prevalence, patient age, and lesion anatomic location.
Differential can be refined by considering clinical history and diagnostic radiologic features, such as pattern of growth, signal intensity, and localization (subcutaneous, intramuscular, intermuscular, etc.).
A systematic approach markedly improves diagnostic results.
Malignancies generally are deep and large.
Only 5% of benign soft tissue tumors exceed 5 cm in diameter.
When sarcomas are superficial, they generally have a less aggressive biologic behavior.
Malignancies usually grow as deep space-occupying lesions, enlarging in a centripetal fashion.
As malignancies enlarge, a pseudocapsule of compressed fibrous connective tissue is formed.
Malignancy is predicted with the highest sensitivity when lesions:
Have a high signal intensity on T2-weighted images.
Are larger than 33 mm in diameter.
Have a heterogeneous signal intensity on T1-weighted images.
Malignancy is predicted with the highest specificity when lesions demonstrate:
Tumor necrosis.
Bone or neurovascular involvement.
Mean diameter of more than 66 mm.
cases based on the morphology of the lesion (6). Criteria used for predicting benign lesions included smooth, well-defined margins, small size, and homogeneous signal intensity, especially on T2-weighted images. Other studies, however, note that malignant lesions may appear as smoothly marginated, homogeneous masses, and MR cannot reliably distinguish benign from malignant processes (2, 3, 4, 5, 7, 37). This discrepancy likely reflects differences within the studied populations, as well as the criteria utilized for their assessment.
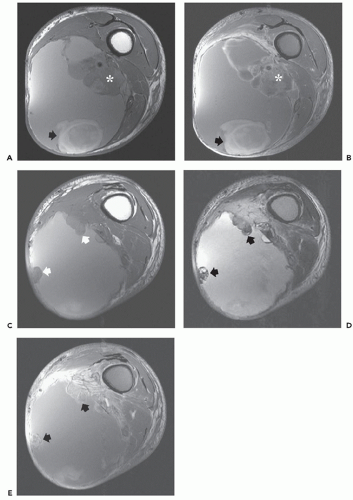 FIGURE 3.8 Hemorrhagic tumor evaluation: Hemorrhagic mass in the leg of a 57-year-old man presenting with a rapidly enlarging thigh mass. Axial T1-weighted (TR/TE; 608/16) (A) and fat-suppressed enhanced T1-weighted (TR/TE; 635/16) (B) spin-echo MR images show a large hemorrhagic mass in the thigh. Note focus of subacute blood posteriorly (arrows) with enhancing viable tumor (asterisk) around superficial femoral artery. Axial T1-weighted (TR/TE; 608/16) (C) and conventional T2-weighted (TR/TE; 2150/80) (D) spin-echo MR images more distally show peripheral nodules (arrows) with intermediate-to-decreased signal intensity. E: Fat-suppressed T1-weighted (TR/TE; 635/16) spin-echo MR image following contrast administration shows enhancement of the nodules (arrows), indicating viable tumor. Biopsy showed highgrade undifferentiated pleomorphic sarcoma. |
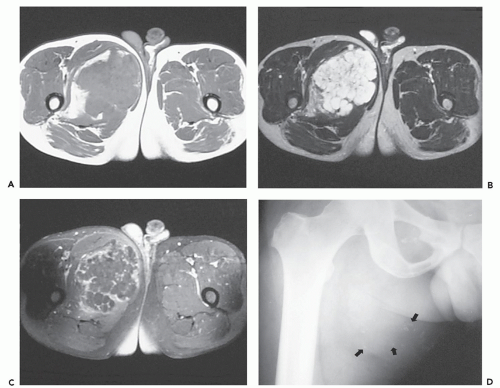 FIGURE 3.9 Cyst mimic: Extra-articular synovial chondromatosis in the thigh of a 35-year-old man, mimicking loculated fluid. A: Axial T1-weighted (TR/TE; 763/18) spin-echo MR image shows large lobulated mass, with signal intensity similar to that of skeletal muscle, in adductor compartment. B: Corresponding conventional T2-weighted (2912/80, TR/TE) spin-echo MR image shows lesion to have signal intensity greater than that of fat. C: Fat-suppressed axial T1-weighted (475/18, TR/TE) spin-echo MR image following contrast administration shows peripheral and septal enhancement, suggesting loculated fluid. D: Radiograph shows nonspecific calcifications (arrows) within mass. |
In the Armed Forces Institute of Pathology (AFIP) series, for example, while 70% of retroperitoneal lesions (for all age groups) were malignant, the malignancy rate for hand and wrist lesions was only 15% (Table 3.3) (67, 68).
TABLE 3.1 Specific diagnoses that may be made or suspected on the basis of MR imaging | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
different from that seen in most primary soft tissue tumors (Fig. 3.13).
TABLE 3.2 Most common lesions by compartment | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||
MR spectroscopy is a noninvasive metabolic imaging technique that has shown value in the identification of malignant tumor markers.
Proton MR spectroscopy is based on the identification of increased choline concentration.
Pooled analysis of previously published studies shows a sensitivity and specificity of 88% and 68%, respectively.
Although spectroscopy is promising, it is technically demanding and there are a number of factors that limit its clinical utility.
TABLE 3.3 Benign and malignant tumor distribution by location and age | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
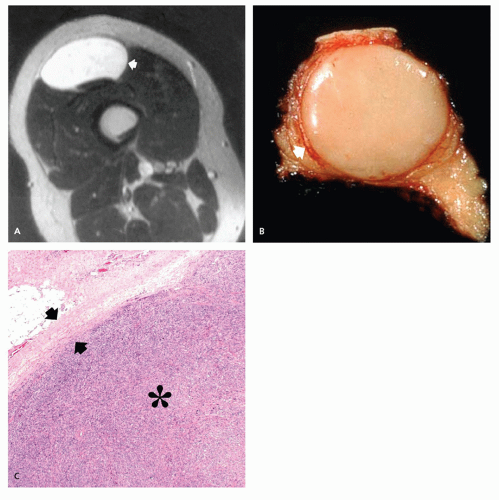 FIGURE 3.10 Pseudocapsule: Myxoid liposarcoma in the thigh of a 26-year-old man. A: Axial T2-weighted (TR/TE; 2000/80) spin-echo MR image shows a homogeneous well-defined mass with an internal cyst-like appearance (arrow). B: Gross photograph from a different patient with a high-grade sarcoma shows the thin pseudocapsule (arrow) at the periphery of the mass. C: High-power photomicrograph shows the pseudocapsule (arrows) at the margin of the sarcoma (asterisk). |
choline a marker for membrane turnover (82). Musculoskeletal imaging has focused on choline concentration, which has been shown to be elevated in malignant tumors (77, 83).
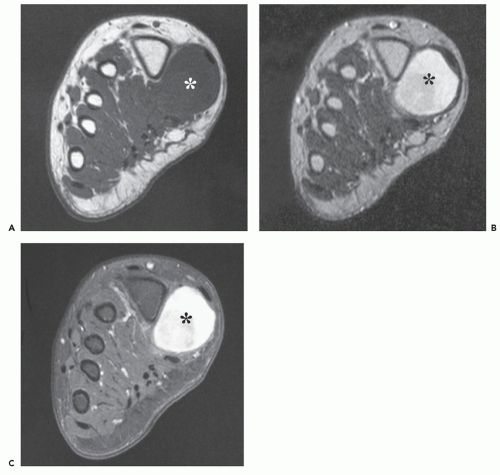 FIGURE 3.11 Well-defined high-grade malignancy with pseudocapsule: Synovial sarcoma in the foot of a 10-year-old girl. Coronal T1-weighted (TR/TE; 450/12) (A) and T2-weighted (TR/TE; 2000/80) (B) spin-echo MR images shows a well-defined mass (asterisk) within the flexor halluces brevis muscle. C: Fat-suppressed axial T1-weighted (TR/TE; 850/12) spin-echo MR image following contrast administration shows intense diffuse enhancement (asterisk). |
musculoskeletal lesions are much more heterogeneous, with greater variation in local field homogeneity (74). In addition, the great variability of coils used to optimize musculoskeletal imaging complicates comparison of quantified results (74).
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


