observed. Swelling of soft tissue, usually fusiform, may be present around involved articulations (see Figs. 6.2A and 6.3E, F); however, periarticular osteoporosis is rarely present. Later in the disease process, bone ankylosis of the phalanges may develop (see Fig. 6.3G). Approximately 15% of patients with erosive osteoarthritis may have clinical, laboratory, and imaging manifestations of rheumatoid arthritis (Fig. 6.4). The exact relationship between these two conditions is still unclear. Some investigators believe that erosive osteoarthritis is actually rheumatoid arthritis originating in unusual sites but subsequently progressing to the articulations that are more typically involved. Others suggest that each is a distinct entity, citing as evidence the fact that the synovial fluid of patients with rheumatoid arthritis does not resemble that of patients with erosive osteoarthritis, that the immunologic abnormalities commonly seen in rheumatoid arthritis are absent in the latter condition, and that the serologic test for rheumatoid factor is negative.
 Figure 6.1 ▪ Inflammatory arthritides. Highlights of the morphology and distribution of arthritic lesions in the inflammatory arthritides. |
Table 6.1 CLINICAL AND IMAGING HALLMARKS OF INFLAMMATORY ARTHRITIDES | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
C-reactive protein, and serum levels of nitrated form of a marker of type II collagen denaturation (Coll2-1NO2) in patients with EOA.
 Figure 6.2 ▪ Erosive osteoarthritis. A: Dorsovolar radiograph of the fingers of both hands of a 51-year-old woman shows characteristic gull-wing erosions of several proximal and distal interphalangeal joints, a configuration resulting from peripheral bone erosion in the distal side of the joint and central erosion in the proximal side of the joint, associated with marginal bone proliferation. Note also accompanied fusiform soft tissue swelling. B: Radiograph of the fingers of both hands of a 49-year-old woman shows typical erosions affecting proximal interphalangeal joint of the middle finger of the right hand and distal interphalangeal joints of both hands. C: Dorsovolar radiograph of the left hand of a 48-year-old woman shows the typical involvement of the proximal and distal interphalangeal joints exhibiting gull-wing pattern. |
joint involvement. Moreover, PA is characterized by other abnormalities not seen in EOA, including skin lesions, nails abnormalities, involvement of sacroiliac joints (sacroiliitis), paraspinal ossifications, and formation of broad-based osteophytes at the plantar aspect of the calcaneus, accompanied by fluffy periostitis. Fluffy periostitis is also seen in the short tubular bones, unlike linear bone apposition observed in EOA. The articular erosions at the DIP joints are also different, with “mouse-ear” rather than “gull-wing” configuration. Lastly, acro-osteolysis and tapered erosions with pencil-like deformities, leading to the so-called arthritis mutilans, are absent in EOA. Although osteophytosis is a consistent phenomenon in EOA, it is almost never seen in RA or PA. When it accompanies the latter conditions, it is secondary because of superimposed degenerative changes rather than a primary feature.
 Figure 6.3 ▪ Erosive osteoarthritis. A: Cone-down view of the index, middle, and ring fingers of a 70-year-old man shows gull-wing erosions of the distal interphalangeal joints. B: Cone-down view of the middle and ring fingers of a 66-year-old woman shows advanced erosions of the proximal interphalangeal joints and early erosions of the distal interphalangeal joints. C: Cone-down view shows characteristic erosion of the proximal interphalangeal joint of the ring finger and distal interphalangeal joint of the index finger of a 53-year-old woman. D: Radiograph of the index and middle fingers of a 50-year-old woman shows gull-wing erosions of the distal interphalangeal joints. |
 Figure 6.3 ▪ (Continued) E: Dorsovolar radiograph of the left thumb of a 51-year-old woman shows characteristic gull-wing erosion of the interphalangeal joint. Note adjacent fusiform soft tissue swelling and lack of periarticular osteoporosis. F: In another patient, a 50-year-old woman, gull-wing erosion is accompanied by periosteal reaction and fusiform soft tissue swelling, very similar to psoriatic arthritis. G: In this patient, a 69-year-old woman, apart from the typical erosions of the proximal interphalangeal joint of the middle finger and distal interphalangeal joint of the index finger, observe also the fusion of the distal interphalangeal joints of the middle and ring fingers. |
those present in EOA. However, differential features include osteopenia, invariably accompanying the changes of hyperparathyroidism, and frequent occurrence of acroosteolysis, a hallmark of former condition. Moreover, the erosions seen in hyperparathyroidism arthropathy are not as sharply demarcated as in EOA, being the result of periosteal, chondral, and subchondral resorption. Other features of hyperparathyroidism, including cortical “tunneling,” “brown” tumors, soft tissue calcifications, and involvement of ligaments and tendons leading to joint laxity and instability, are additional differentiating features.
 Figure 6.4 ▪ Progression of erosive osteoarthritis into rheumatoid arthritis. A: Dorsovolar radiograph of the hand of a 58-year-old woman demonstrates the gull-wing configuration of erosive changes in the proximal interphalangeal joints and the distal interphalangeal joint of the small finger. Because of protracted pain and lack of response to conservative treatment, she underwent joint resection followed by implantation of silicone-rubber prostheses in the proximal interphalangeal joints of the index, middle, and ring fingers, together with fusion of the interphalangeal joint of the thumb and the distal interphalangeal joint of the small finger. Five years after surgery, the classic radiographic features of rheumatoid arthritis developed, involving the wrists (B), elbows, shoulders, hips, and cervical spine. Note the surgical fusion of interphalangeal joints of the thumb and fifth finger, as well as the spontaneous fusion of the distal interphalangeal joints of the index and ring fingers. |
Although it is much enigmatic, most rheumatologists also include under the rubric of “rheumatoid arthritis” a condition called seronegative rheumatoid arthritis (see text below), in which patients present without rheumatoid factor or antibodies to CCP but with the clinical and imaging picture of rheumatoid arthritis. Currently, rheumatoid arthritis is considered to be a heterogeneous autoimmune disorder, with genetic factors playing an important role in the disease expression. Multiple genome-wide association studies have been conducted, but the results have generally been disappointing. The genetics is complex and multifactorial and varies between ethnic populations. The best association is with the major histocompatibility complex (MHC), but the data have yielded no practical clues that can be translated to the bedside. Although the association with the susceptibility loci of HLA-DRB1 (which encodes the β-chain of HLA-DR) and PTPN22 genes is better understood, several non-HLA loci have been linked to this arthritis, including the 18q21 chromosome region of the TNFRSR11A gene, which encodes the receptor activator of nuclear factor kappaB. In addition, a common genetic variant at the TRAF1-C5 locus on chromosome 9 is associated with an increased risk of anti-CCP-positive rheumatoid arthritis. Allelic variants of HLA-DRB1 associated with risk for rheumatoid arthritis encode a similar sequence, namely, amino acids 70 to 74, known as the shared epitope (SE). The detection of antibodies to citrullinated proteins (CCP), representing specific autoantibodies in the patient’s serum, is an important diagnostic finding.
 Figure 6.5 ▪ Rheumatoid arthritis of the hip joints. A: Anteroposterior radiograph of the pelvis of a 47-year-old woman shows uniform narrowing of both hip joints accompanied by axial migration of the femoral heads. B: Anteroposterior radiograph of the right hip of a 60-year-old woman with advanced rheumatoid arthritis shows concentric joint space narrowing, with axial migration of the femoral head leading to acetabular protrusion. Some superimposed secondary osteoarthritic changes are also present. C: Anteroposterior radiograph of the left hip of a 64-year-old woman shows erosions of the femoral head and acetabulum, concentric narrowing of the hip joint, and acetabular protrusion. |
addition, cephalad migration of the humeral head may be seen secondary to destructive changes in the shoulder joint and rupture of the rotator cuff (Fig. 6.8A); resorption of the distal end of the clavicle, which assumes a pencil-like appearance, may also be observed. Tear of the rotator cuff in this condition (Fig. 6.8B, C) must be differentiated from the chronic traumatic form of this abnormality (Fig. 6.9). In the knee joint, all three compartments are commonly narrowed in a uniform manner (Fig. 6.10). The loss of the articular cartilage is caused by inflammation and pannus formation. There is little evidence of bone repair or osteophyte formation, and there is invariably associated joint effusion (Fig. 6.11). In the elbow and ankle, uniform joint space narrowing is observed (Figs. 6.12, 6.13, 6.14).
 Figure 6.6 ▪ MRI of rheumatoid arthritis of the hip joint. Coronal proton density-weighted fat-suppressed MRI (A) and coronal proton density-weighted fat-suppressed MR image (B) of the right hip joint of a 31-year-old woman obtained after intravenous administration of gadolinium show uniform narrowing of the joint space, joint effusion, synovitis, and erosions of the femoral head and acetabulum. |
 Figure 6.7 ▪ Rheumatoid arthritis of the shoulder joint. Radiograph of the left shoulder of a 70-year-old woman shows periarticular osteoporosis and concentric narrowing of the glenohumeral joint. |
 Figure 6.8 ▪ Rheumatoid arthritis, chronic rotator cuff tear. A: Anteroposterior radiograph of the right shoulder of a 72-year-old man with advanced rheumatoid arthritis shows upward migration of the humeral head secondary to rotator cuff tear, a common complication of rheumatoid changes in the shoulder joint. Note the characteristic tapered erosion of the distal end of the clavicle, erosions of the humeral head, and the substantial degree of periarticular osteoporosis. Coronal oblique (B) and sagittal (C) proton density-weighted fat-suppressed MR images of the left shoulder of a 64-year-old woman show large articular and periarticular erosions, joint space narrowing, joint effusion, and a tear of the supraspinatus tendon (arrows), all the features of advanced rheumatoid arthritis. |
or intrabursal loose bodies are commonly associated with rheumatoid arthritis and are thought to represent a complication of chronic inflammatory process. Occasionally, they also may be seen in seronegative inflammatory arthritis and even in tuberculous arthritis. These particles contain collagen, fibrinogen, fibrin, reticulin, elastin, mononuclear cells, blood cells, and some amorphous material (Fig. 6.23). On radiography (Fig. 6.24), this condition occasionally can be mistaken for synovial chondromatosis (see Chapter 10). On MR T1-weighted images, rice bodies exhibit intermediate signal intensity, whereas on T2 weighting, they are only slightly hyperintense relative to muscle (Figs. 6.25 and 6.26).
 Figure 6.9 ▪ Massive posttraumatic rotator cuff tear. A: Coronal oblique proton density-weighted fat-suppressed MR arthrographic image of the right shoulder of a 32-year-old man, who sustained multiple injuries in a motorcycle accident, shows a full-thickness tear of the supraspinatus tendon (arrow). The supraspinatus muscle is medially retracted (open arrow). B: More posterior section shows also a tear of the infraspinatus tendon (arrow). Note lack of inflammatory features seen in rheumatoid arthritis. |
 Figure 6.10 ▪ Rheumatoid arthritis of the knee joints. Anteroposterior (A) and lateral (B) radiographs of the right knee of a 52-year-old woman joints show tricompartmental involvement. Note the periarticular osteoporosis, joint effusion, and lack of osteophytosis. Anteroposterior (C) and lateral (D) radiographs of both knees of a 50-year-old man show uniform narrowing of the medial, lateral, and femoropatellar joint compartments associated with joint effusions. |
 Figure 6.11 ▪ MRI of rheumatoid arthritis of the knee. Coronal T1-weighted (A) and coronal proton density-weighted (B) fat-suppressed MR images of the left knee of a 50-year-old woman show uniform joint space narrowing of the lateral and medial compartments, destruction of the articular cartilage, subchondral bone erosions, and tear of the lateral and medial menisci. C: Coronal T1-weighted MRI of the right knee of another patient demonstrates a joint effusion with inflammatory pannus (arrow). Note the lower signal intensity of the fluid as compared to the slightly higher signal of the pannus. |
 Figure 6.12 ▪ Rheumatoid arthritis of the elbow joint. Anteroposterior (A), lateral (B), and radial head-capitellum (C) views of the elbow of a 61-year-old woman show narrowing of the joint spaces, erosions of the subchondral bone of the capitellum, radial head, and trochlea, and joint effusion, manifested by the positive anterior and posterior fat-pad sign (arrows). |
 Figure 6.13 ▪ MRI of rheumatoid arthritis of the elbow joint. Coronal T1-weighted (A), coronal inversion recovery (IR) (B), and coronal (C) and sagittal (D) T1-weighted fat-suppressed MR images of the elbow joint of a 52-year-old woman, obtained after intravenous injection of gadolinium, show extensive synovitis, joint effusion, and articular erosions. |
 Figure 6.14 ▪ Rheumatoid arthritis of the ankle joints. Anteroposterior (A) and lateral (B) radiographs of the ankle show uniform joint space narrowing of the tibiotalar, subtalar, Chopart, and Lisfranc joints. |
 Figure 6.15 ▪ Rheumatoid arthritis of the hip joint. Anteroposterior radiograph of the left hip of a 59-year-old woman with advanced rheumatoid polyarthritis demonstrates the typical erosions of the femoral head and acetabulum, and acetabular protrusio. Note the lack of osteophytosis and the only very minimal reactive sclerosis. |
affected. This latter point, however, is controversial, because some investigators believe that if the distal interphalangeal joints are involved, the condition may represent juvenile idiopathic arthritis or another form of polyarthritis, not classic rheumatoid arthritis.
 Figure 6.16 ▪ Rheumatoid arthritis: osseous erosions. A: Lateral radiograph of the heel of a 49-year-old woman shows retrocalcaneal bursitis (arrow) without osseous erosions. B: Lateral radiograph of the foot of a 55-year-old woman who presented with a heel pain shows fluid in the retrocalcaneal bursa (arrow) associated with erosion of the calcaneus (curved arrow). C: Sagittal STIR MR image in another patient demonstrates bone erosion in the posterior process of the calcaneus (arrowhead) associated with extensive surrounding bone marrow edema and retrocalcaneal and retro-Achilles bursitis (arrows). D: Sagittal T1-weighted fat-saturated postcontrast MRI of the ankle in another patient demonstrates a large tibiotalar joint effusion with enhancing synovium/pannus. Note the bone erosions in the talus and navicular bones containing enhancing inflammatory pannus (arrows). |
 Figure 6.17 ▪ Rheumatoid arthritis: osseous erosions. Norgaard view of both hands of a 33-year-old woman shows early erosions of both pisiform bones (arrows). |
 Figure 6.18 ▪ Rheumatoid arthritis: osseous erosions. A: Dorsovolar radiograph of both hands of a 50-year-old woman shows erosion of the right triquetral bone (arrow). This was an isolated osseous abnormality in this patient. Coronal proton density-weighted (B) and coronal proton density-weighted (C) fat-suppressed MR images demonstrate erosion of the triquetrum associated with soft tissue edema (arrows). Note also edema in adjacent extensor carpi ulnaris tendon (arrowheads). D: Transverse US image of the same area also effectively depicts the triquetral erosion (arrow). |
 Figure 6.19 ▪ PET/CT of osseous erosion. Axial and coronal reformatted fused 18F-FDG PET/CT images of the right wrist of a 59-year-old woman with rheumatoid arthritis show high glucose uptake in the pisiform-triquetral compartment and erosion of the triquetral bone (arrows). |
 Figure 6.20 ▪ Rheumatoid cyst. Anteroposterior radiograph of the left knee of a 35-year-old woman with rheumatoid arthritis shows a large synovial cyst in the proximal tibia. Note also articular erosions and periarticular osteoporosis. |
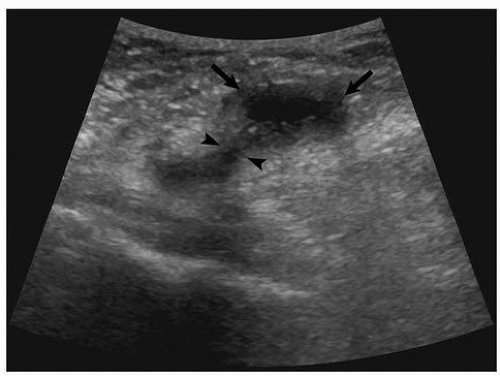 Figure 6.21 ▪ US of the Baker cyst. Transverse US image of the knee of a 42-year-old woman with rheumatoid arthritis shows an oval in shape hypoechoic area (arrows) that communicates with the knee joint (arrowheads). |
 Figure 6.22 ▪ MRI of the Baker cyst. Sagittal (A) and axial (B) T2-weighted fat-suppressed MR images of a 60-year-old woman with rheumatoid arthritis demonstrate a large popliteal cyst (arrows). Open arrows point to erosive changes of the articular cartilage; curved arrows indicate joint effusion. |
 Figure 6.23 ▪ Rice bodies. Photograph of fibrinous loose bodies recovered from the knee joint of the patient with rheumatoid arthritis. (From Bullough PG. Atlas of Orthopedic Pathology with Clinical and Radiologic Correlation. 2nd ed. New York, NY: Gower Medical Publishing; 1992, Fig. 11.18, p. 11.6.) |
 Figure 6.24 ▪ Rice bodies. Anteroposterior radiograph of the right shoulder of a 60-year-old woman with advanced rheumatoid arthritis demonstrates multiple rice bodies within subacromial-subdeltoid bursae complex. |
 Figure 6.25 ▪ MRI of rice bodies. Oblique coronal proton density-weighted (A), sagittal proton density-weighted (B), and oblique coronal T2-weighted (C) fat-suppressed MR images of the left shoulder of a 66-year-old woman with rheumatoid arthritis show numerous rice bodies within the shoulder joint. |
 Figure 6.26 ▪ MRI of rice bodies. Sagittal (A) and axial (B) fast spin-echo (FSE) proton density-weighted fat-suppressed MR images of the right knee of a 68-year-old woman with rheumatoid arthritis show numerous rice bodies within the joint fluid (arrows). |
 Figure 6.27 ▪ Rheumatoid nodules. A: Lateral radiograph of the right elbow of a 39-year-old man demonstrates erosions of the olecranon process (arrow), olecranon bursitis (open arrow), and rheumatoid nodules on the dorsal aspect of the forearm (curved arrows). Note the characteristic pitlike cortical erosions at the site of the rheumatoid nodules (arrowheads). B: A 68-year-old woman with rheumatoid arthritis had a large rheumatoid nodule at the lateral side of the elbow joint. Note erosions at the radiocapitellar joint (arrow). |
 Figure 6.28 ▪ MRI of very early changes of rheumatoid arthritis. Coronal STIR MR image of the hand demonstrates bone marrow edema involving the proximal phalanx and distal metacarpal of the second digit, with prominent periarticular soft tissue edema. Bone marrow edema may be seen on MRI before the bone erosions are seen on radiographs (pre-erosive edema). This feature makes MRI a good tool for establishing an early diagnosis thus leading to early therapy of rheumatoid arthritis. |
 Figure 6.29 ▪ MRI of tenosynovitis. Two axial STIR (A, B) and axial T1-weighted fat-suppressed (C) MR postcontrast images of the wrist of a 67-year-old woman with rheumatoid arthritis show synovial thickening and diffuse tenosynovitis of all flexor and extensor tendons. |
 Figure 6.30 ▪ US of small joint synovitis. A: Longitudinal ultrasound image of the left second metacarpophalangeal joint of a 60-year-old man with rheumatoid arthritis shows hypoechoic triangular area at the site of distended joint capsule, representing joint effusion and synovial thickening. B: Power Doppler color scale of the same area shows increased vascularity consistent with synovial hyperemia from active inflammation. (Reprinted with permission from Klein MJ, Bonar SF, Freemont T, et al., eds. Atlas of Nontumor Pathology. Non-neoplastic Diseases of Bones and Joints. Washington DC: American Registry of Pathology and Armed Forces Institute of Pathology, 2011, Fig. 2-17, p. 68.) |
 Figure 6.31 ▪ US and MRI of tenosynovitis. Longitudinal (A) and transverse (B) US images of the anterior aspect of the left ankle of a 65-year-old woman with rheumatoid arthritis show markedly thickened anterior tibialis tendon and fluid within the tendon sheath (arrows). C: Sagittal T1-weighted MR image confirms the thickening of the anterior tibialis tendon. D: Axial proton density-weighted fat-suppressed MR image shows in addition fluid within the anterior tibialis tendon sheath (arrows) and tenosynovitis of the peroneus longus and brevis tendons. |
 Figure 6.32 ▪ Rheumatoid arthritis—loss of articular cortex. A: Very early radiographic feature is the loss of so-called articular cortex of the metacarpal head on the radial aspect (arrow). Compare with the intact outline of the normal third and fourth metacarpal heads. B: In another patient, the metatarsal heads are affected in similar manner (arrows), but to a slightly greater extent. |
 Figure 6.33 ▪ Rheumatoid arthritis—erosions in bare areas. Invasion of inflammatory pannus (P) into the articular areas not covered by the articular cartilage (so-called bare areas) causes marginal erosions (arrows). |
radial deviation of the wrist in the radiocarpal articulation (Fig. 6.43). In far-advanced stages of rheumatoid arthritis, shortening of several phalanges may be encountered secondary to destructive changes in the joints associated with dislocations in the metacarpophalangeal joints. This deformity appears as a “telescoping” of the fingers, hence its name, main en lorgnette, from the French name for the telescoping type of opera glass (Fig. 6.44). An abnormally wide space between the lunate and the scaphoid may also be encountered in advanced stages of the disease secondary to erosion and rupture of the scapholunate ligament (Fig. 6.45); this phenomenon is known in the literature as the Terry-Thomas sign. Joint deformities are also often seen in the foot, and subluxation in the metatarsophalangeal joints often leads to deformities such as hallux valgus and hammer toes (Fig. 6.46).
 Figure 6.34 ▪ Rheumatoid arthritis—erosions in bare areas. A: Typical erosions in the bare areas are seen in this 55-year-old woman with rheumatoid arthritis. Note also periarticular osteoporosis and soft tissue swelling. B: Radiograph of the index finger shows erosion in the bare area at the base of the proximal phalanx (arrow) associated with soft tissue swelling. C: Radiograph of the middle finger of another patient shows erosions in the bare areas at the distal end of the proximal phalanx (arrows). |
 Figure 6.35 ▪ Rheumatoid arthritis of the hands. A: Dorsovolar radiograph of both hands of a 63-year-old woman shows typical for this disease loss of articular cartilage and subchondral erosions affecting predominantly metacarpophalangeal, radiocarpal, and intercarpal joints. Observe that the distal interphalangeal joints are spared. B: Dorsovolar radiograph of both hands of a 72-year-old woman shows articular erosions affecting metacarpophalangeal joints of both hands. The proximal interphalangeal joints of the left hand are also affected. The distal interphalangeal joints are normal. |
 Figure 6.36 ▪ CT of rheumatoid arthritis of the wrist. Coronal (A) and sagittal (B) reformatted CT images of the left wrist of a 39-year-old woman show erosions of the radiocarpal joint and erosions of the several carpal bones. |
 Figure 6.37 ▪ MRI of rheumatoid arthritis of the wrist. Coronal (A) and axial (B) T1-weighted fat-suppressed MR images of the right wrist of a 60-year-old woman, obtained after intravenous administration of gadolinium, show erosions of the ulnar styloid and several carpal bones including the scaphoid, lunate, triquetrum, capitate, and hamate. There are also erosions of the second and third carpometacarpal joints. Note in addition extensive synovitis exhibiting high signal intensity. |
 Figure 6.38 ▪ Rheumatoid arthritis of the feet. Dorsoplantar radiograph of both feet of a 55-year-old woman shows erosions and subluxations of metatarsophalangeal joints. |
 Figure 6.39 ▪ MRI of rheumatoid arthritis of the foot. Long-axis T1-weighted (A), long-axis proton density-weighted fat-suppressed (B), and short-axis T1-weighted fat-suppressed (C) postcontrast MR images of the left foot of a 64-year-old woman show erosions of the second, third, and fourth metatarsophalangeal joints (arrows) accompanied by synovitis. |
 Figure 6.40 ▪ CT of rheumatoid arthritis of the foot. A and B: Two sagittal reformatted CT images of the hindfoot of a 52-year-old man show erosions of the subtalar and calcaneocuboid joints.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





