Introduction
Intensity-modulated proton therapy (IMPT) can begin only after a number of other processes have been completed, including simulation and treatment planning. For both proton and photon treatments, radiation oncology has evolved to the point in which the treatment parameters, defined in the treatment planning process, are included in the radiation oncology electronic medical record (EMR) to be uploaded to the delivery system for each treatment field on each day. At the completion of daily treatment for a specific patient, the delivery system downloads a number of parameters of the treatment delivered on that day. The delivery system may also have its own logs, which contain a history of operations at specific times on a specific day. These treatment delivery logs are the ultimate source of truth because they record the details as to the actions taken by the treatment device. It is necessary on limited occasions to consult the treatment logs to confirm the individual treatment on a specific day.
IMPT is an example of a very complex treatment technique that would be impossible to deliver without the use of an EMR to upload the treatment parameters. In addition to the treatment parameters, patient-specific referenced images are also uploaded to the delivery system so that a comparison can be made to daily patient setup images. It is not unusual that there are devices or systems from multiple vendors involved in the IMPT treatment process. For example, at MD Anderson Cancer Center (MDACC), the treatment delivery system is provided by vendor H (Hitachi), the EMR system by vendor E (Elekta), and the treatment planning system (TPS) by vendor V (Varian). A key to this successful digital communication is the Digital Imaging and Communications in Medicine (DICOM) standard. DICOM was developed by the American College of Radiology and the National Electrical Manufacturers Association to aid the distribution and viewing of medical images. The first version of DICOM was released in 1985. DICOM for radiation therapy came later, in 1995, with DICOM Working Group 7. Information on this industry standard can be found on the DICOM homepage, dicom.nema.org . DICOM is a very successful, mature standard that has evolved over time and continues to evolve. DICOM makes IMPT possible in the multivendor environment.
DICOM defines many basic radiation therapy ion beam attributes, including beam type (static or dynamic), radiation type (photon, proton, ion), scan mode (none, uniform, modulated, modulated spec), and so on. DICOM uses the concept of control points for radiation therapy treatments. Control point 0 has the cumulative meter set weight set to zero and defines all initial parameters (e.g., gantry, table, collimator). Control points are important in IMPT delivery. A new control point is defined for each energy change. Each control point has a specific number of spots and monitor units (MUs).
Treating with individual spots (packets of protons), which change energy and location, is different than treating with large fields, either protons or photons. The concept of dose, energy deposited per unit mass, needs reflection when treating with spots; for example, the unit mass involved and the instantaneous dose rate. One potential unique catastrophic failure would be the corruption of data or failure of devices such that all spots were delivered to the same physical location over and over and over.
Intensity-modulated proton therapy treatment delivery
IMPT is a highly conformal radiation treatment in which the intensity of the proton beam is adjusted and shaped to conform to the shape and depth of the tumor. Individual spots of the pencil proton beam can have different energies, different locations, and different intensities (dose). IMPT offers a three-dimensional (3D) approach to sculpt the radiation pattern to match the target.
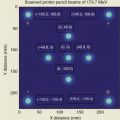
In 2008, Hitachi provided University of Texas MD Anderson Cancer Center (UT MDACC) Proton Therapy Center in Houston the second clinical spot scanning system in the world. The first clinical spot scanning facility is the Paul Scherrer Institute, a multidisciplinary research institute in Switzerland. Some 94 different proton energies are available with ranges from 4.0 to 30.6 cm. The maximum field size is 30 cm × 30 cm. The maximum MU per spot is 0.04 MU, whereas the minimum MU per spot is 0.005 MU. The full width at half maximum spot size in air at isocenter varies from 12 to 34 mm, depending on the energy. MDACC chose to define the MU in a manner consistent with photon MU definitions, as opposed to the number of protons passing through the dose monitor approach. The definition of the MU was built into the TPS early in the commissioning process.
The MDACC spot scanning nozzle has a very conservative design, as appropriate for an early system. The length of the beam path in the nozzle is greater than 3 m. As the beam enters the nozzle, the beam encounters the profile monitor and then enters a helium chamber. Outside of the helium chamber, there is the Y scanning magnet and then the X scanning magnet. Eventually, the beam passes through two dose monitors and a spot position monitor. Before leaving the nozzle, the beam can pass through an energy filter (ridge filter) and an energy absorber (range shifter), if such devices are in place. Finally, it is possible to insert an aperture for the purpose of reducing the penumbra. The system has worked well for the treatment of patients with discrete spot scanning proton therapy, including the IMPT technique.
Routine patient IMPT delivery requires a treatment plan that contains parameters for each spot (beam energy, location, and the MU/dose per spot), a record and verify/EMR, which uploads the treatment parameters to the delivery system and records the treatment delivered, and the delivery system. Table 7.1 displays treatment field parameters for a multifield optimized treatment plan with three treatment fields for a head and neck patient.
| Prescription Isodose Line (%) | CTV60 (cc) | Total Target (cc) | Field | Nominal Range (cm) | Nominal SOBP (cm) | Max E (MeV) | Layers | Total Spots | mu |
| 100.0 | 32.2 | 201.4 | ALPPB BPAPB CLAPB | 10.2 20.3 7.5 | 10.2 18.6 7.4 | 153.2 203.7 143.2 | 37 47 32 | 1973 1910 3144 | 62.94 60.94 109.46 |
At MDACC, the current TPS system is Eclipse from Varian, the EMR system is Mosaiq from Elekta, and the delivery system is from Hitachi. The software associated with each system may change or may remain static. Substantial testing is required when there is a change in software. In the last 10 years, there have been upgrades to Eclipse at approximately 2-year (or longer) intervals and upgrades in Mosaiq at approximately 18- to 24-month intervals. There have been no changes in the Hitachi system delivery system software. This stability in the treatment delivery control system is reassuring, to a point, as upgrades are useful to refine the treatment process. In a large clinic, changes in the radiation oncology practice-wide EMR may be driven by developments outside of protons, which are only supported by newer versions of the EMR software.
Radiation oncology has now evolved to the point at which nearly all patients are treated using the radiation oncology EMR, even emergent patients. Approximately more than 9000 patients have been treated at the UT MDACC proton center, including approximately 3000 spot scanning patients. Zero patients have been treated without the use of the Rad Onc EMR. This enforces a safety discipline on treatment delivery because there are no last-minute rush patients. Before the first fraction is treated, clinical physics must approve the calibration and the chart after reviewing the initial quality assurance (QA) measurements.
The Hitachi treatment delivery system can deliver the beam while in three different modes, namely, treatment mode, physics mode, and service mode. The number of active interlocks changes in the various modes. Service mode is essentially limited to service and almost exclusively used for service purposes. Physics mode is designed for the physicists to perform commissioning, patient-specific and machine QA. The parameters for physics mode tests are stored in folders that are not contained in the EMR. In physics mode, it is easy to run the same file multiple times. In treatment mode, all interlocks are functional, and all field-specific parameters must be uploaded from the EMR each time that the field is run and downloaded from the delivery system after each delivery. Time is required for this information transfer, in addition to the time required to deliver the proton beam. For protons, Mosaiq EMR has a special function for each treatment field, entitled QA. This function is used to upload to Mosaiq the field strength of the last bending magnet so that this parameter can be verified for each treatment. Doses are not recorded in the EMR when Mosaiq QA is used. Patient treatment field delivery using the Mosaiq QA option with the Hitachi system in treatment mode must be performed for each field before patient treatments can be delivered.
Verification of the treatment parameters is performed independently in the Hitachi delivery system and in a joint fashion between the Hitachi system and Mosaiq. The details are important regarding which information is available in which system. For example, the TPS provides the energy of the proton beam required to treat the required depth. The delivery system needs to provide the correct energy from the accelerator and set the correct beam optics parameter to have the desired energy to exit the nozzle. For photons, there is one beam energy per field, for example, 6 MV. For IMPT, there are multiple beam energies per field, for example, 33 different beam energies. The nozzle beam optics must be changed for each beam energy. Thus, the verification of the magnetic field strength for the final gantry bending magnet is an important check to ensure that the delivered spot is appropriate.
Treatment mode of the Hitachi system is not very efficient for physics to deliver the same field multiple times to measure the dose distribution at various depths as part of the pretreatment patient QA process. Thus this part of patient-specific QA work is performed in physics mode. The communication within the Hitachi delivery system between the treatment mode and the physics mode is nonexistent, so the same patient information must be communicated in a different manner, outside of the EMR. The current method of transferring information from the TPS to the treatment device in physics mode is through the use of a memory stick, which is an old-fashioned approach and frowned on by information security.
Both therapists and physicists must interact with the Hitachi system through the human-machine interface. There are three major phases in this interaction, namely, the download phase, the setup phase, and the irradiation phase. Verification in the Hitachi system has two different components, namely, the clinical verification and machine verification. Clinical verification confirms that the verify switch is IMPAC (now called Mosaiq) and that certain basic parameters have been set, including patient, gantry, dose monitor, and 6 degrees of freedom (DOF) couch. The machine verification displays the status of very specific machine parameters that are required to deliver the treatment. Treatments begin with the therapist first interacting with the EMR and downloading patient treatment parameters to the delivery system. The delivery system must internally confirm certain parameters and communicate their correct settings back to the EMR before the next steps can be taken in the delivery system. There is a constant communication check between the EMR and the delivery system.
Treatments do not always proceed as expected in that the treatment delivery system may abort itself during treatment because of electronic noise or encountering some unexpected setting. The ability to recover correctly from an unexpected abort during an IMPT treatment is important. With our system, when an abort occurs and treatments are only partially delivered, the Hitachi system uploads to Mosaiq the number of control points and spots per control point that have been delivered. This is accurate to within one spot. The Mosaiq system has the ability to record the partial treatment and then calculate the remaining control points and spots that remain to be delivered. This partial plan can then be downloaded back to the delivery system and the remaining treatment delivered. MDACC has developed additional software that analyzes the Hitachi logs in the event of an abort. This software provides an independent tool to review the performance of the delivery system and to focus on conditions that may be causing the system to abort during treatments. These conditions include the name of the field being delivered, the gantry angle, and the specifics regarding control points and spot numbers. The exact point where the system aborted (beam energy, spots delivered at this energy) is easily determined. This MDACC-developed software, which sends emails to both proton physics and the Hitachi service and maintenance leaders, is much easier to use and much quicker than reviewing the Hitachi logs. The number of aborts per day varies over the years depending on the conditions of the system. Currently, the system is aborting once or twice per day. Recovery to deliver the remaining dose of a partially treated field could be changeling in treatment mode. The accelerator and EMR vendors are encouraged to optimize the delivery work flow, including recovery of partial treatment. It should be remembered that the inability to deliver the entire spot pattern will result in a portion of the target volume receiving less than the daily prescribed dose. This is different than the situation with scattered protons or photons in which the entire treatment volume may receive less than the desired dose.
In summary, IMPT treatment requires that, before treatment, each treatment field is run to upload specific treatment parameters from the delivery system to the EMR system. Thus QA must always be performed before the first treatment. Generally, but not always, IMPT treatment delivery works well, assuming that the required steps are taken in order. The delivery system does occasionally abort. There are established mechanisms for partial treatment with EMR and treatment delivery system.
Every patient has their own specific IMPT treatment plan. The treatment plan generally has more than one field. Each field has a number of proton energies. Each energy has a number of different spots. Each spot has a specific location and a certain dose (MUs) to be delivered. The net result from each field is a 3D dose pattern, which can be highly modulated. The TPS provides a dose pattern based upon the patient’s anatomy. Generally, the first step in patient-specific QA is to convert the dose pattern in the patient to a dose pattern in water phantom. Three-dimensional dosimetry systems are in active development but are not in routine use at MDACC. There are well-established 2D ion chamber array dosimetry systems in routine use, for example, the MatriXX. Multiple 2D measurements can be made to approximate the 3D dose pattern, or measurements can be made at only one depth, which will confirm the spot pattern at that depth. Table 7.2 displays the results of measurements made with the MatriXX versus calculations using a 3%/3-mm dose-distance agreement criteria. Some 90% or more of the pixels passed this criterion.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


