Leukodystrophies
ADRENOLEUKODYSTROPHY
KEY FACTS
Most important peroxisomal disorder which is characterized by very long-chain fatty acids that are not metabolized and are elevated in serum and other body fluids.
The neonatal type is rare and due to multiple enzyme deficiencies; it involves the white matter diffusely.
The X-linked type is more common (>80%) and is due to a single enzyme defect (lignoceroyl CoA ligase leading to accumulation of very long-chain fatty acids); it presents in males 4 to 8 years of age (hearing and visual defects, loss of developmental milestones); neurologic symptoms precede adrenal insufficiency in a majority of cases; a vegetative state or death usually occurs 2 years after onset of symptoms.
In 80% of patients, imaging shows bilateral and symmetrical demyelination in occipitoparietal regions with an enhancing margin at the front; auditory pathways and the splenium corpus callosum may be involved.
Early in the disorder, only the corticospinal tracts or the lateral lemnisci may be affected.
Magnetic resonance spectroscopy shows high choline and low N-acetyl-aspartate at enhancing “front,” low choline, creatine, and NAA and high myoinositol at areas of chronic involvement.
DTI may show to a better extent the degree of white matter involvement.
Main differential diagnosis: none; findings are typical in this age group.
 FIGURE 16-1. Axial FLAIR image shows symmetrical high signal in posterior white matter and splenium. |
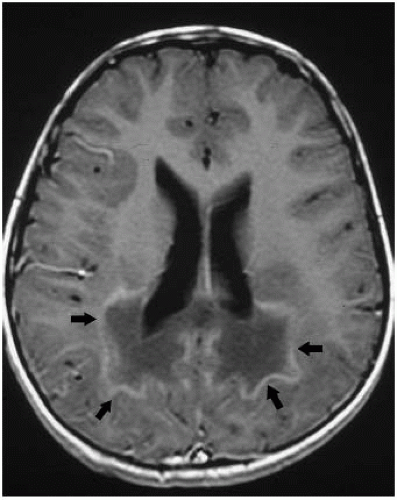 FIGURE 16-2. Postcontrast axial T1, in the same patient, shows enhancement in margins (arrows) of white matter lesions. |
SUGGESTED READING
Schneider JFL, Il’yasov KA, Boltshauser E, Hennig J, Martin E. Diffusion tensor imaging in cases of adrenoleukodystrophy: preliminary experience as a marker for early demyelination? Am J Neuroradiol 2003;24:819-824.
METACHROMATIC LEUKODYSTROPHY
KEY FACTS
Lysosomal disorder characterized by a deficiency of arylsulfatase A, which results in the accumulation of sulfatides and is toxic to white matter.
Most common inherited leukodystrophy (1:100,000 newborns).
Most patients present between 1 and 2 years of age; juvenile and adult forms of the disease also exist; most common type of adult-onset leukodystrophy.
Imaging studies show diffuse white matter disease; magnetic resonance imaging shows sparing of subcortical U-fibers and areas of increased T2/fluid attenuated inversion recovery (FLAIR) signal intensity in cerebellum. Sparing of perivascular white matter may give rise to “tigroid” appearance.
MRS shows moderately high choline, low NAA, and high myoinositol. Diffusion-weighted imaging may show restricted diffusion in areas of abnormal high T2/FLAIR signal.
End-stage disease is indistinguishable from other leukodystrophies by imaging studies.
Death occurs 1 to 4 years after onset of symptoms.
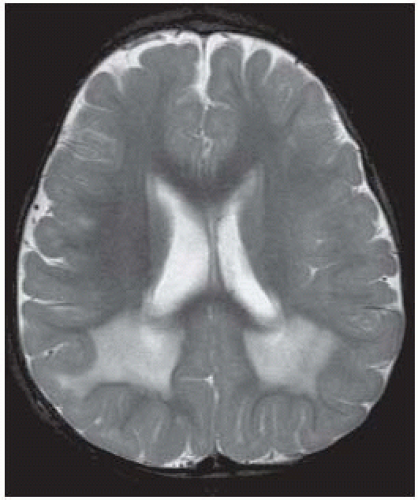 FIGURE 16-3. Axial T2 shows symmetrical high signal in posterior white matter with sparing of subcortical regions. |
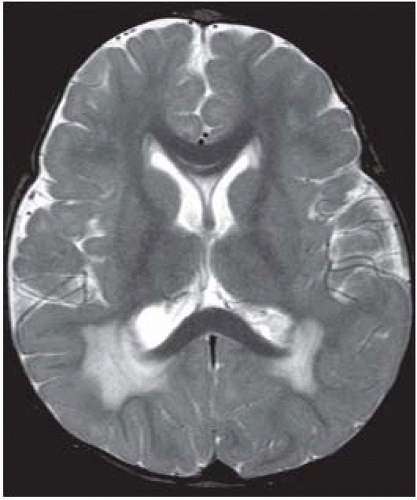 FIGURE 16-4. Axial T2, in the same patient, shows abnormal high signal in white matter of occipital lobes with sparing of subcortical regions and splenium. |
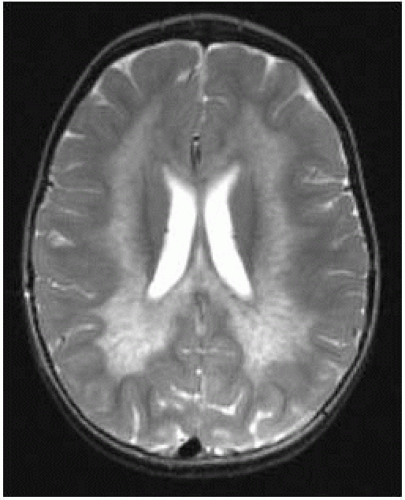 FIGURE 16-5. Axial T2, in a different patient, shows more extensive white matter involvement but sparing of subcortical U-fibers. |
 FIGURE 16-6. Axial T2, in a different patient, shows typical tigroid appearance of white matter that contains residual myelinated regions. |
SUGGESTED READING
Kim TS, Kim 10, Kim WS, Choi YS, Lee JY, Kim OW, et al. MR of childhood metachromatic leukodystrophy Am J Neuroradiol 1997;18:733-738.
van der Voorn JP, Pouwels PJW, Kamphorst W, Powers JM, Lammens M, Barkhof F, et al. Histopathologic correlates of radial stripes on MR images in lysosomal storage disorders. Am J Neuroradiol 2005;26:442-446.
ALEXANDER DISEASE
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


