Metabolic Disorders
AMINO ACID DISORDERS
KEY FACTS
In this rare group of disorders, amino acid pathways are deficient, and proteolipids, which are essential for formation of myelin, are abnormal.
Phenylketonuria is caused by defective phenylalanine hydroxylase, producing increased phenylalanine, which inhibits a proteolipid, leading to dysmyelination; patients are normal at birth and MRI shows nonspecific white matter changes that may be more obvious on DWI.
Maple syrup disease is characterized by a failure to metabolize branched-chain amino acids; it presents in the neonatal period and is rapidly fatal; white matter, basal ganglia, and particularly brain stem and internal capsules are involved and show restricted ADC acutely.
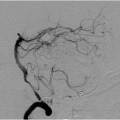
Homocystinuria is due to an error in methionine metabolism, which leads to abnormal collagen and elastin formation and presents as multiple arterial and venous occlusions.
Glutaric aciduria type 1 typically results in dilatation of sylvian fissures (not true arachnoid cysts) and high T2/FLAIR signal in basal ganglia and hemispheric white matter.
Other rare aminopathies include methylmalonic acidemia (symmetrical involvement of globus pallidi), nonketotic hyperglycinemia, and oculocerebrorenal (Lowe) syndrome.
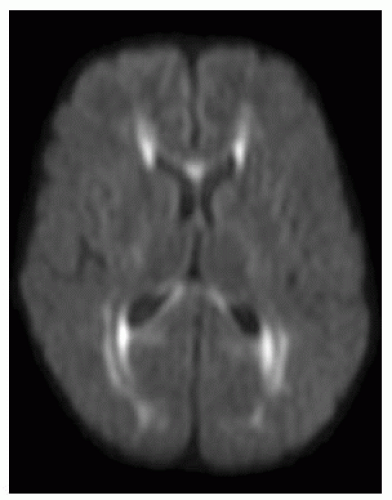 FIGURE 17-1. Axial DWI shows high signal in periventricular regions, along optic radiations, and in the corpus callosum in an adult with phenylketonuria. |
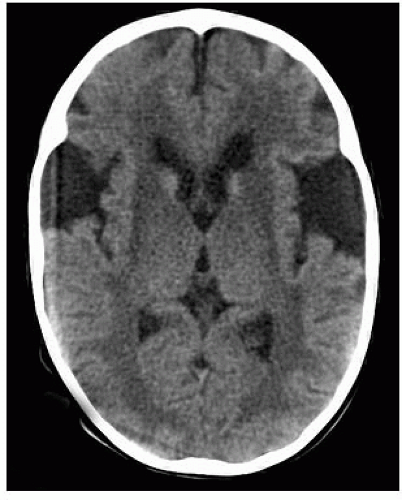 FIGURE 17-2. Axial CT shows wide sylvian fissures and low density in basal ganglia in a child with glutaric aciduria type 1. |
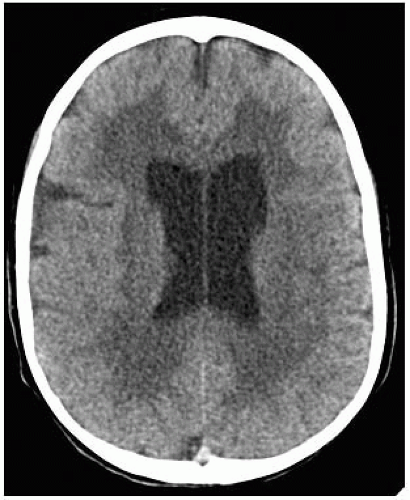 FIGURE 17-3. Axial CT, in the same patient as 17-2, shows prominent lateral ventricles and diffuse white matter hypodensity. |
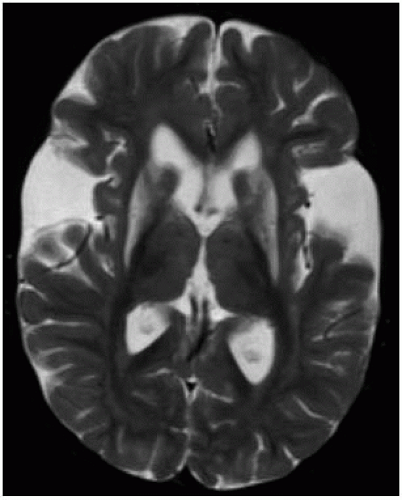 FIGURE 17-4. Axial T2, in a different patient, shows wide sylvian fissure and abnormal high signal in basal ganglia bilaterally. |
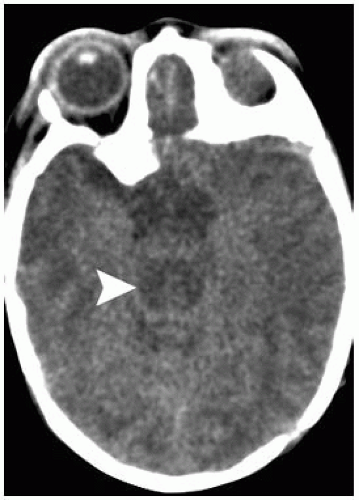 FIGURE 17-5. Axial CT, in a patient with maple syrup urine disease shows hypodense and swollen brain stem (arrowhead). |
 FIGURE 17-6. Axial CT, in the same patient, shows hypodense and swollen midbrain (arrowheads). |
 FIGURE 17-7. Axial DWI, in a different patient, shows high signal in the midbrain and corticospinal tracts in a patient with maple syrup urine disease. (Case courtesy A. Vidal, Chile.) |
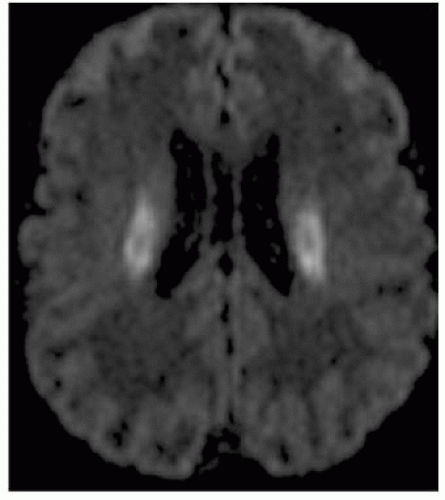 FIGURE 17-8. Axial DWI in the same patient as 17-7 showing high signal in the posterior corticospinal tracts (all abnormalities had restricted ADC values). |
SUGGESTED READING
Okamoto K, Tokiguchi S, Furusawa T, Ishikawa K, Quardery AF, Shinbo S, et al. MR features of diseases involving bilateral middle cerebellar peduncles. Am J Neuroradiol 2003;24:1946-1954.
Peng SSF, Tseng WYI, Chien YH, Hwu WL, Liu HM. Diffusion tensor images in children with early-treated, chronic, malignant phenylketonuric: correlation with intelligence assessment. Am J Neuroradiol 2004;25:1569-1574.
MUCOPOLYSACCHARIDOSES
KEY FACTS
Disorders characterized by deficiencies in the metabolism of heparan, dermatan, and keratan sulfate.
Disorders include Hurler (IH), Hunter (II), Sanfilippo (III A-D), Morquio (IV A-D), Maroteaux-Lamy (VI), Scheie (IS), and Sly syndromes.
All mucopolysaccharidoses are autosomal recessive except Hunter, which is X-linked.
All mucopolysaccharidoses involve the CNS and musculoskeletal system.
Findings are usually nonspecific and range from mild to severe white-matter abnormalities, communicating hydrocephalus, initial macrocephaly (all are microcephalic chronically), cerebral atrophy, dilatation of perivascular spaces, thick skull, thick dura, abnormal odontoid, and thick posterior longitudinal ligament in spine (particularly cervical region).
MRS: mildly high choline, low NAA with a peak at 3.7 ppm, which may be related to sugars that are a part of mucopolysacharides.
Main differential diagnosis: tuberous sclerosis, Canavan, Lowe disease.
 FIGURE 17-9. Axial FLAIR image in a patient with Hurler disease shows increased signal throughout white matter and dilated perivascular spaces. |
 FIGURE 17-10. Parasagittal T1, in the same patient, shows dilated perivascular spaces in the corpus callosum and ventricular dilatation. |
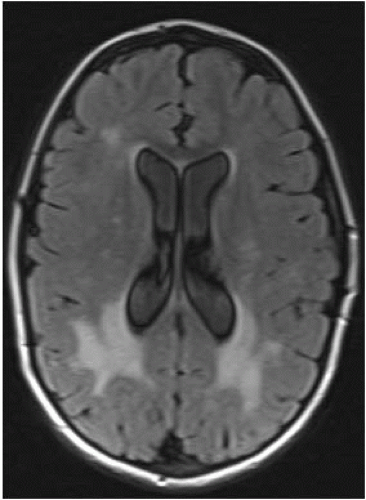 FIGURE 17-11. Axial FLAIR, in a different patient, shows mildly prominent lateral ventricles and abnormal white matter posteriorly (Hunter disease). |
 FIGURE 17-12. Axial FLAIR in a patient with advanced Hunter’s shows diffuse white matter abnormalities, dilated perivascular spaces, and cortical atrophy.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|