KEY FACTS
Terminology
- •
Mucinous epithelial neoplasm, which can be benign (mucinous cystadenoma), borderline (low malignant potential), or malignant (mucinous cystadenocarcinoma)
Imaging
- •
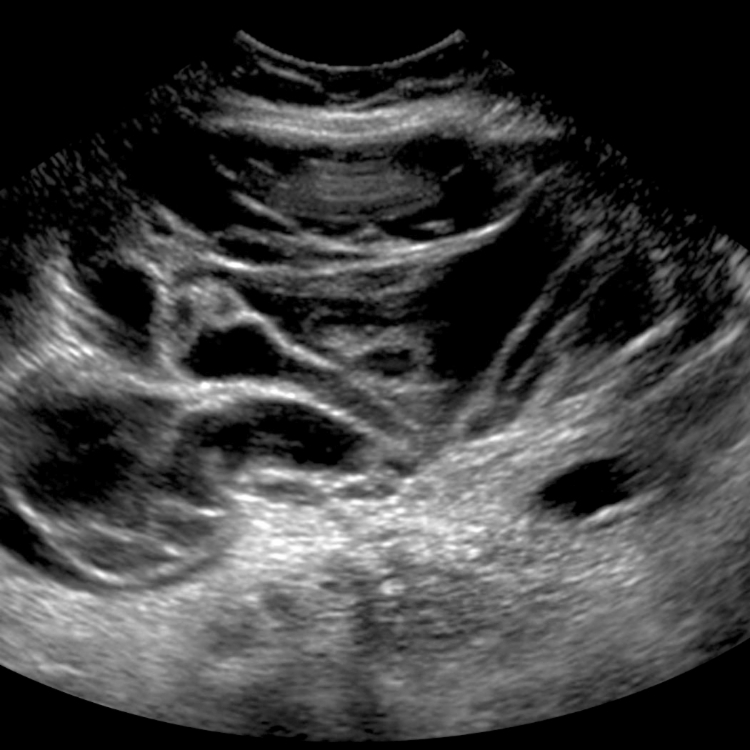
Multilocular cystic mass with low-level echoes
- ○
Mucin creates low-level echoes within loculi
- –
Echogenicity can be variable depending on concentration of mucin
- –
- ○
Papillary projections much less common than in serous tumors
- ○
Solid components increase suspicion for malignancy
- ○
- •
Variable in size but often large; may fill entire pelvis and extend into upper abdomen
- •
Pseudomyxoma peritonei is potential form of peritoneal spread
- ○
More echogenic than simple ascites
- ○
Amorphous, mucoid material insinuating itself around mesentery, bowel, and solid organs
- ○
Has mass effect with scalloping along solid organs (especially liver) and bowel matted posteriorly (rather than free-floating)
- ○
Top Differential Diagnoses
- •
Endometrioma
- •
Serous cystadenoma/carcinoma
Pathology
- •
Method of spread
- ○
Intraperitoneal dissemination most common (pseudomyxoma peritonei)
- ○
Direct extension to surrounding organs
- ○
Lymphatic spread to paraaortic and pelvic nodes
- ○
Clinical Issues
- •
Massive tumors can cause weight gain and distended abdomen
- •
CA-125 not useful for mucinous tumors: False-negative in 30%
- •
Mucinous tumors 2nd most common epithelial neoplasm
- •
Gelatinous, insinuating nature of pseudomyxoma peritonei makes complete resection difficult
Scanning Tips
- •
Mucinous tumors are less commonly malignant than serous tumors