Musculoskeletal System
QUESTIONS
1 Where does Tc-99m MDP localize within the bone?
A. Osteoblast
B. Osteoclast
C. Osteoid matrix
D. Calcium hydroxyapatite
View Answer
1 Answer D. Bone composition can be divided into mineralized and unmineralized portions. Mineral phase of the bone is composed of two-thirds crystalline hydroxyapatite and one-third noncrystalline calcium phosphate. Derivatives of bisphosphonates such as Tc-99m MDP and Tc-99m HDP as well as F-18 NaF localize within the hydroxyapatite portion of the bony matrix by chemical adsorption (chemisorption); extraosseous uptake of these radiopharmaceuticals such as that in myositis ossificans may occur in calcium phosphate portion of the matrix. Radiochemicals such as P-32 mainly localize within the noncrystalline calcium phosphate portion of the bony matrix. The unmineralized portion of the bone is composed of osteoid (organic portion of the bone matrix that forms prior to maturation of bone tissue, i.e., collagen, etc.) and cellular components such as osteoblast, osteoclast, and marrow.
References: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:272.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:98.
2 Excessive aluminum in the technetium generator eluate during the preparation of Tc-99m MDP will result in localization of the radiopharmaceutical in which of the following organs?
A. Brain
B. Stomach
C. Lungs
D. Liver
View Answer
2 Answer D. Excessive aluminum from the generator elution causes colloid formation, which can accumulate in the liver. Causes of diffuse abnormal hepatic activity on bone scan include the following: excessive aluminum in elution from generator, residual activity from a previous sulfur colloid scan, excessive serum aluminum, hepatic necrosis, hepatic metastases, amyloidosis, and metastatic calcifications.
References: MacDonald J. Idiopathic hepatic uptake of 99mTc methylene diphosphonate: a case report. J Nucl Med Technol 2001;29(1):32-36.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:98.
3 Injection of excessive air into the mixing vial during the preparation of Tc-99m MDP will result in radiopharmaceutical localization in which of the following organs?
A. Brain
B. Stomach
C. Lungs
D. Liver
View Answer
3 Answer B. Excessive air in the mixing vial will result in oxidation of tin from stannous ion (Sn II) to stannous hydroxide (Sn IV). This will cause poor tagging of the radiopharmaceutical and will result in excessive free pertechnetate. Free pertechnetate can also be visualized if the radiopharmaceutical injection is delayed for more than 4 hours after its preparation. Free pertechnetate localizes within the salivary glands, thyroid gland, and stomach and increases the background soft tissue activity. As such, quality control with chromatography should be routinely performed before the injection of the radiopharmaceutical to ensure greater than 95% binding.
References: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:271.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:98.
4 A “four-phase bone scintigraphy” typically involves additional imaging at what time point?
A. 2 to 3 hours
B. 4 to 10 hours
C. 6 to 12 hours
D. 18 to 24 hours
E. 22 to 28 hours
View Answer
4 Answer D. Sometimes, 18- to 24-hour images are performed after intravenous administration of Tc-99m-labeled bisphosphonate in a patient with renal failure or in a patient who has poor soft tissue clearance. This is termed the fourth phase. In a “three-phase” study, the images are acquired during an angiogram phase (first), soft tissue perfusion/blood pool phase (second), and delayed 2- to 3-hour phase (third). Three-phase imaging is typically utilized in differentiating osteomyelitis from cellulitis or soft tissue infection. It is also positive in fracture or malignancy. Other indications for three-phase bone scintigraphy include evaluation of painful joint prosthesis and complex regional pain syndrome (reflex sympathetic dystrophy).
References: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:273.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:100.
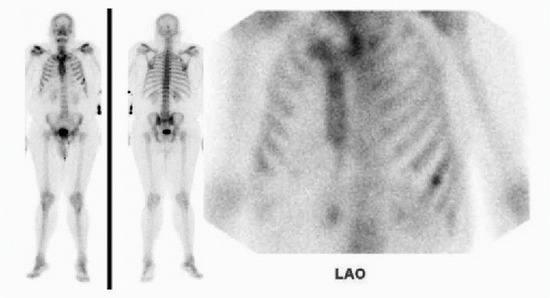
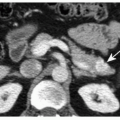
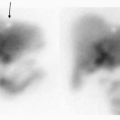
5 A 65-year-old male with newly diagnosed high-risk prostate cancer (Gleason score 7 + 8) presents for initial staging with bone scintigraphy. The patient denies any history of pain and denies history of recent or remote trauma. Based on the supplied images, what is the most appropriate next step?
 |
A. Correlation with PSA level
B. Correlation with chest x-ray
C. Correlation with CT
D. Correlation with MRI
View Answer
5 Answer C. A single focus of intense radiopharmaceutical uptake is noted within the left seventh rib. An isolated rib lesion is rarely attributable to metastasis (according to Wang and Shen only 1.2%). However, in the absence of any clinical history of recent or remote trauma, further correlation with additional imaging should be considered. CT scan would be the most appropriate test to characterize this lesion. Chest x-rays are not sensitive in evaluation of suspected rib metastasis. While serum PSA may or may not be elevated, it will not be able to answer the cause of abnormal rib uptake.
Correlation with this patient’s CT scan of the abdomen and pelvis done earlier on the same day demonstrated presence of a sclerotic lesion within the anterolateral aspect of the left seventh rib (arrow below). Absence of callous formation, lack of cortical discontinuation, or lack of history of trauma suggested that this was less likely to be a sequela of fracture. Since it was the only site of involvement, this was later biopsied and confirmed to be a prostatic metastasis. Positive finding on bone scintigraphy is nonspecific and may represent sequela of malignancy, trauma, or infection. Careful correlation with clinical history and appropriate anatomic imaging is crucial for an accurate diagnosis. Of note, a typical rib metastasis is oblong and tracks along the rib as seen in a bone scan from a different patient below. Fractures are typically seen as vertically aligned foci of increased uptake in several successive ribs.
 |
Reference: Wang C, Shen Y. Study on the distribution features of bone metastases in prostate cancer. Nucl Med Commun 2012;33(4):379-383.

A. Renal failure
B. Normal study
C. Diffuse metastasis
D. Hypertrophic osteoarthropathy
View Answer
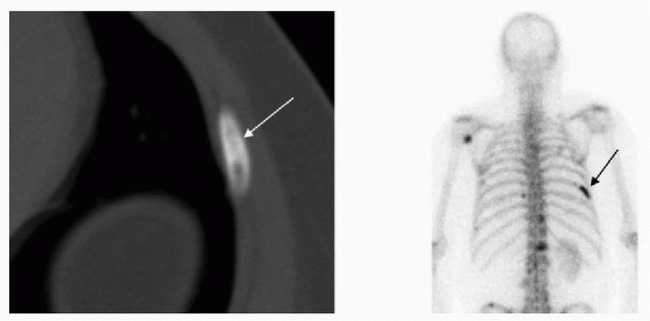
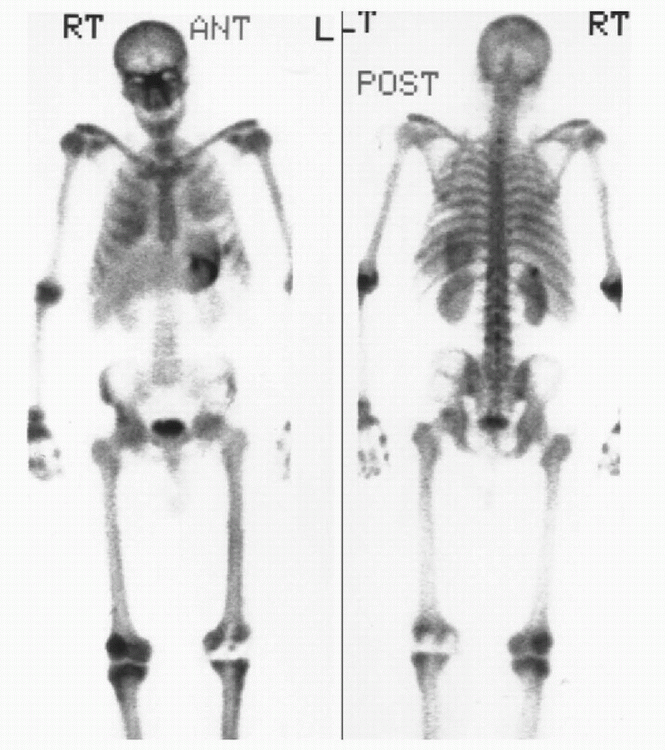
6 Answer C. Normal physiologic distribution of the radiotracer on the bone scan includes the GU system, and attention to the kidneys should be paid on the bone scan. The supplied images demonstrate diffusely increased radiotracer uptake throughout the spine, pelvis, ribs, and the proximal appendicular skeleton with absent visualization of the kidneys. The findings are most compatible with a superscan. The kidneys are not visualized on the superscan due to intense uptake within the osseous structures. If these images were windowed down, renal parenchyma would be more evident. Superscan is most commonly secondary to osseous metastatic disease; however, it can also be seen with metabolic disorders such as primary hyperparathyroidism, renal osteodystrophy, myelofibrosis, mastocytosis, and hypervitaminosis D. A patient with renal failure would demonstrate more background soft tissue uptake on 3-hour delayed images secondary to decreased clearance of the radiotracer. An 18- to 24-hour delayed “fourth-phase” scan in patients with renal failure/dialysis may produce similar appearance and is often referred to as a “beautiful scan.” Superscan or beautiful scan associated with primary hyperparathyroidism and renal osteodystrophy (secondary hyperparathyroidism) often demonstrates increased radiotracer uptake within an enlarged mandible, which is referred to as a “Lincoln sign,” as well as increased uptake within periarticular bones. Hypertrophic osteoarthropathy typically demonstrates increased radiotracer uptake within the periosteum of long bones, which is often referred to as “tram tracking.”
References: Habibian, MR. Nuclear medicine imaging: a teaching file, 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2009:326-328.
Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:267, 279, 291.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:99, 106.
A. Paget disease
B. Osteosarcoma
C. Osteomyelitis
D. Fibrous dysplasia
E. Ewing sarcoma
F. Severely comminuted fracture
View Answer
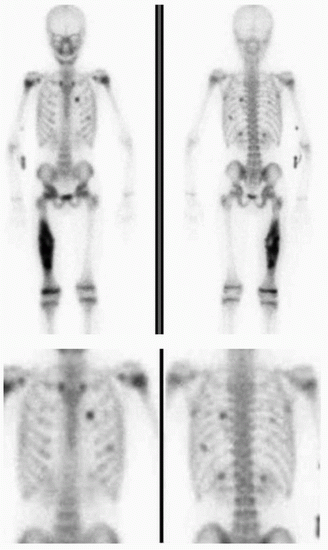
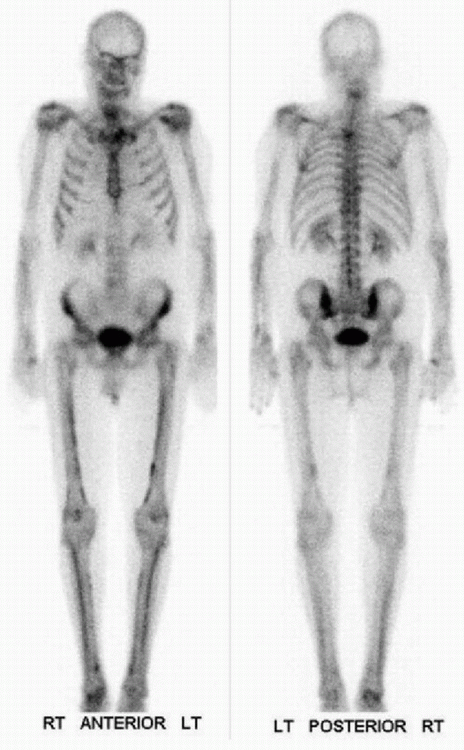
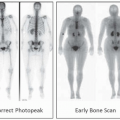
7 Answer B. Delayed anterior and posterior whole-body images demonstrate a large focus of intense radiotracer uptake within the right femoral diaphysis. Multiple small foci of intense radiotracer uptake are seen within the right and left chest, which do not correspond to locations of the ribs (arrow below). The findings are most compatible uptake within lung metastasis, typically seen with osteosarcoma. In questionable cases, SPECT-CT may be performed to confirm the location of metastasis in the lungs. Lung metastasis from osteosarcoma demonstrates intense bisphosphonate radiotracer uptake due to presence of ossification within the metastasis. While diaphyseal location is typically associated with Ewing sarcoma, lung metastasis from Ewing sarcoma would not be expected to demonstrate intense Tc-99m MDP uptake. Osteosarcoma commonly arises from the distal femoral metaphysis and demonstrates heterogeneous uptake containing areas of photopenia (see image from a different patient below). While osteomyelitis may occur in femoral diaphysis, it will typically demonstrate well-defined, homogeneous increase in radiotracer uptake. Both osteomyelitis and osteosarcoma would be positive on three-phase bone scintigraphy.
 |
References: Mebarki M, Medjahedi A, Menemani A, et al. Osteosarcoma pulmonary metastasis mimicking abnormal skeletal uptake in bone scan: utility of SPECT/CT. Clin Nucl Med 2013;38(10):e392-e394.
Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:285-288.
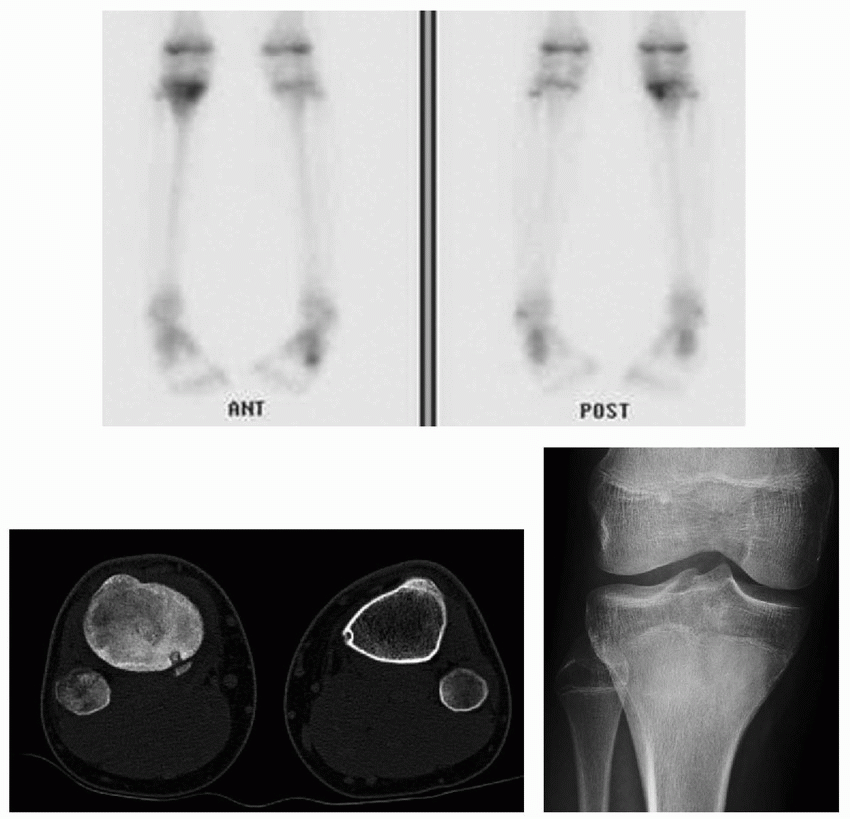
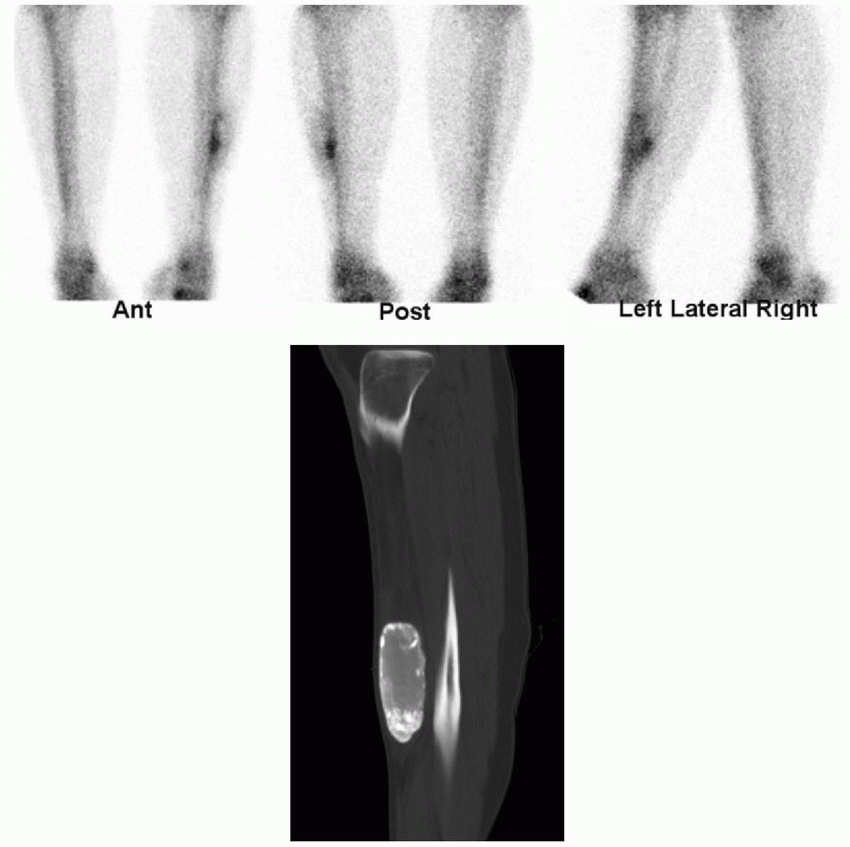
8 A 12-year-old boy presents with severe right knee pain that is worse at night. Based on the following scintigraphic and CT findings, what is the most likely diagnosis?
 |
A. Stress fracture
B. Bone island
C. Osteosarcoma
D. Osteoid osteoma
E. Metastatic neuroblastoma
View Answer
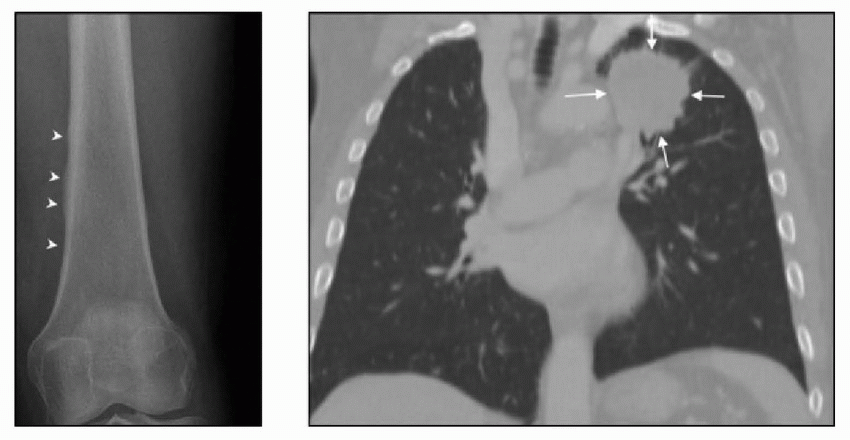
8 Answer D. A small round focus of intense uptake (arrow) in the posteromedial aspect of the proximal tibia is surrounded by a more diffuse mild uptake in the proximal tibial metaphysis (arrowheads). The radiograph demonstrates diffuse sclerosis within the proximal tibial metadiaphysis with solid (nonaggressive) periosteal reaction laterally. CT demonstrates a well-defined round low-attenuation nidus (black arrowheads) with a central area of high attenuation/mineralization (white arrow) within the posteromedial tibial cortex. The combination of these findings is most compatible with an osteoid osteoma. Osteoid osteoma is more common in femur and tibia (>50%) with less common sites including spine, hands, and feet (30%). The least common locations include the skull, scapula, ribs, pelvis, mandible, and patella.
Osteomyelitis would have a more homogenous appearance on bone scintigraphy and lack a hyperintense nidus. Stress fracture would demonstrate linear intense uptake without surrounding mild uptake. Bone islands rarely accumulate MDP. Osteosarcoma would appear more diffuse as well and would be expected to have aggressive periosteal reaction (sunburst appearance) on radiograph and CT. This is the wrong age group for metastatic neuroblastoma.
 |
Reference: Chai JW, Hong SH, Choi JY, et al. Radiologic diagnosis of osteoid osteoma: from simple to challenging findings. Radiographics 2010;30(3):737-749.
9 Which of the following primary osseous lesions usually demonstrates normal activity on bone scintigraphy?
A. Osteoblastoma
B. Osteoid osteoma
C. Fibrous dysplasia
D. Giant cell tumor
E. Cortical desmoid
View Answer
9 Answer E. Osteoblastomas, osteoid osteoma, fibrous dysplasia, and giant cell tumors usually demonstrate intense activity on delayed bone scintigraphy. Chondroblastomas may demonstrate moderate or intense activity. Enchondromas can demonstrate mild to moderate activity. Fibrous cortical defects and nonossifying fibromas typically demonstrate normal or mild uptake. Cortical desmoid tumors, bone island, and hemangioma usually demonstrate normal activity on the bone scan. It is important to recognize that benign primary bone neoplasms may demonstrate abnormal uptake as they are usually incidentally found on the bone scintigraphy. The specific diagnosis of benign primary bone tumors is usually dependent on their radiographic appearance.
Reference: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:281-285.
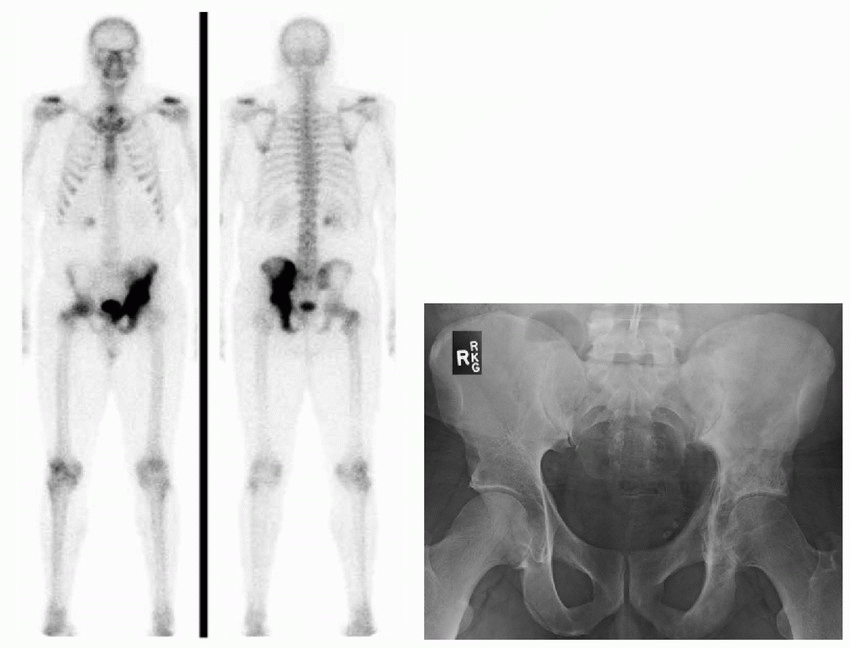
10 A 56-year-old male with history of prostate cancer presents for further evaluation with bone scintigraphy in the setting of elevated alkaline phosphatase levels. Based on the bone scan and pelvic radiograph images, what is the most likely diagnosis?
 |
A. Metastasis
B. Fibrous dysplasia
C. Paget disease
D. Osteosarcoma
View Answer
10 Answer C. Anterior and posterior delayed whole-body images demonstrate intense radiotracer uptake within the left hemipelvis involving the left ilium, ischium, and pubic bones in a contiguous fashion. The correlating radiograph demonstrates asymmetric bone expansion, cortical (iliopectineal and ilioischial lines) thickening (arrows below), and coarsened trabeculae. The findings are most compatible with Paget disease. Frequent sites of Paget involvement include pelvis (30% to 75%), spine (30% to 75%), skull (25% to 65%), and proximal long bones (25% to 30%). Less commonly affected sites include shoulder girdle and forearm. Polyostotic disease (65% to 90%) is more frequent than monostotic disease (10% to 35%). Pelvic involvement is more often asymmetric than symmetric.
Three phases of Paget are described. Early resorptive phase is characterized by lysis and thinned cortex. Descriptors such as “blade of grass” and “osteoporosis circumscripta” are seen in this phase. The lytic phase is followed by the mixed phase characterized by coarsening and thickening of trabeculae and cortex. Majority of the cases seen by radiologist are in the mixed phase. The mixed phase later progresses to the final blastic phase at variable rate. Due to increased blood flow and bone turnover, lytic and mixed phases are typically characterized by intense uptake on bone scintigraphy. The more quiescent late blastic phase may show normal radionuclide uptake. Sarcomatous transformation of Paget is rare, occurring in approximately 1% of cases, and is seen as focal bone destruction extending through the cortex with an associated soft tissue mass.
Fibrous dysplasia may also demonstrate similar degree of intense radiopharmaceutical uptake. However, it is typically seen in young patients (75% present by age 30) and can be distinguished from Paget disease based on the pattern of involvement and radiographic findings. While Paget disease involves the end of the bone, fibrous dysplasia typically does not involve the epiphysis. Contiguous involvement of the hemipelvis would be atypical for metastasis. The supplied radiograph also excludes metastasis and osteosarcoma as possibilities.
Reference: Smith SE, Murphey MD, Motamedi K, et al. From the archives of the AFIP. Radiographics 2002;22(5):1191-1216.
11 Which of the following statements is LEAST accurate regarding nuclear medicine imaging of complications related to hip replacement?
A. Activity surrounding a cemented prostheses resolves within 1 year.
B. Diffuse increase in activity surrounding the stem suggests hardware infection.
C. Focal increase in activity at the tip and intertrochanteric regions suggests hardware loosening.
D. F-18 FDG-PET imaging is the method of choice for evaluation of suspected prosthetic infection.
View Answer
11 Answer D. Activity surrounding a cemented prosthesis usually returns to normal within 12 months after surgery. On the other hand, generalized increased activity may be seen for more than 2 years after surgery with a noncemented, porous-coated prosthesis. Persistent activity at the tip of the femoral shaft component and at the trochanter may represent hardware loosening, while a generalized increase in activity around a hip prosthesis, especially the stem, may indicate osteomyelitis. Combined labeled leukocyte-marrow imaging is the radionuclide study of choice for diagnosing prosthetic joint infection. Accuracy of F-18 FDG-PET is lower than that of the combined labeled leukocyte-marrow imaging.
References: Kwee TC, Kwee RM, Alavi A. FDG-PET for diagnosing prosthetic joint infection: systematic review and metaanalysis. Eur J Nucl Med Mol Imaging 2008;35(11):2122-2132.
Love C, Marwin SE, Palestro CJ. Nuclear medicine and the infected joint replacement. Semin Nucl Med 2009;39(1):66-78.
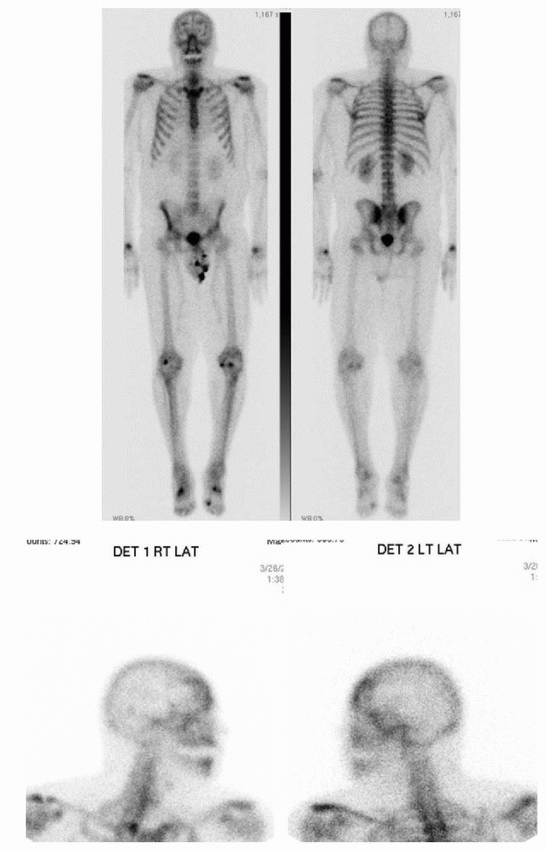
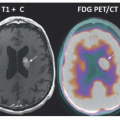
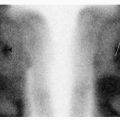
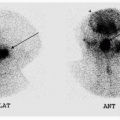
12 The following bone scan is from a 76-year-old male with castration-resistant prostate cancer and rising PSA. What is the most likely explanation for the findings in the skull?
 |
 |
A. Metastasis
B. Meningioma
C. Paget disease
D. Fibrous dysplasia
E. Hyperostosis frontalis
View Answer
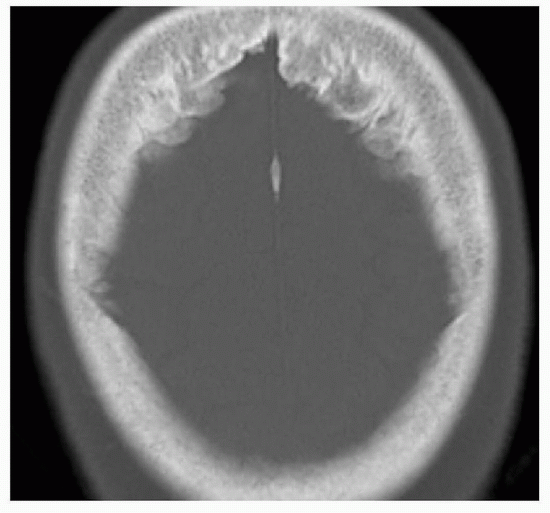
12 Answer E. Delayed anterior and posterior whole-body images demonstrate increased uptake in the head, which localizes to the frontal bone on the lateral spot views. Single axial CT scan demonstrates symmetric overgrowth of the inner table of frontal bones. These findings are most compatible with hyperostosis frontalis. This is a benign process and should not be confused with malignancy. Paget disease would be evidenced by focal lysis (osteoporosis circumscripta) during the lytic phase or sclerotic diploic expansion and thickened cortices during mixed/blastic phase with an appearance likened to “cotton wool.” Metastasis or “en plaque” meningioma-related hyperostosis would not be symmetric. Fibrous dysplasia would be seen in younger population and would demonstrate medullary expansion with “ground-glass” matrix on CT scan. While this case was in a man, hyperostosis frontalis is far more common in women.
Reference: Novetsky GJ, Berlin L. Bone scintigraphy in hyperostosis frontalis interna. Clin Nucl Med 1982;7(6):265-266.
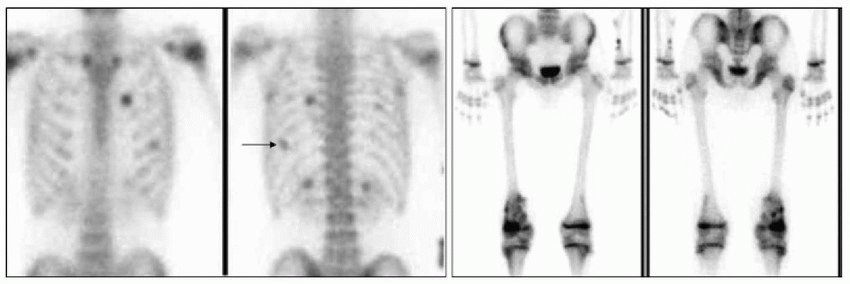
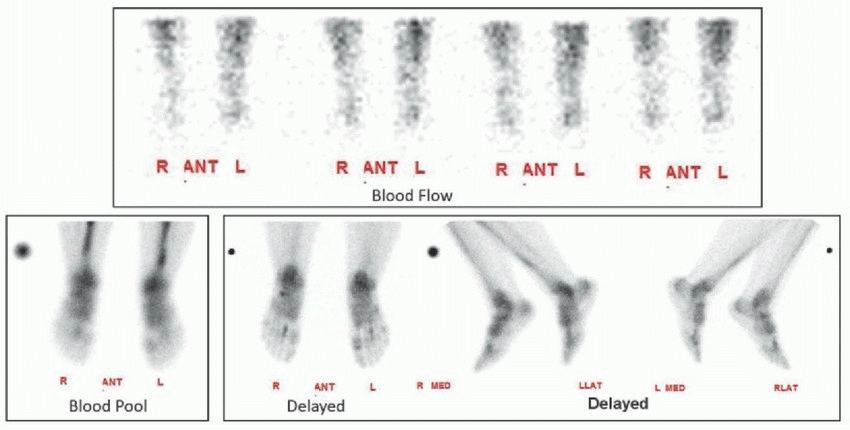
13 The following 65-year-old female presents with bilateral feet pain. Based on the three-phase scintigraphy images of the feet, what is you conclusion?
 |
A. Complex regional pain syndrome
B. Multifocal osteomyelitis
C. Insufficiency fractures
D. Plantar fasciitis
E. Normal study
F. Cellulitis
View Answer
13 Answer C. The anterior blood flow and blood pool images show focal areas of hyperemia and hyperperfusion in the region of the right distal second and left distal third metatarsals. Delayed images show further localization of the radiopharmaceutical in those locations. These findings are most compatible with multiple acute fractures. Given that there is no history of trauma, they likely represent insufficiency fractures related to osteopenia or alendronate-induced pathologic metatarsal fractures. Insufficiency fractures are secondary to normal stress on abnormal bone, while fatigue stress fractures are a result of abnormal stress on a normal bone. Focal increased activity in the left first metatarsophalangeal joint on the delayed image is consistent with osteoarthritis. Plantar fasciitis would demonstrate increased activity at the insertion of the plantar fascia along the anterior inferior calcaneus. Complex regional pain syndrome would demonstrate increased blood flow and blood pool to the affected extremity with increased periarticular radiotracer uptake on the delayed phase. Cellulitis would only be positive on the first two phases, and uptake associated with osteomyelitis would be less focal.
Reference: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:296-300.
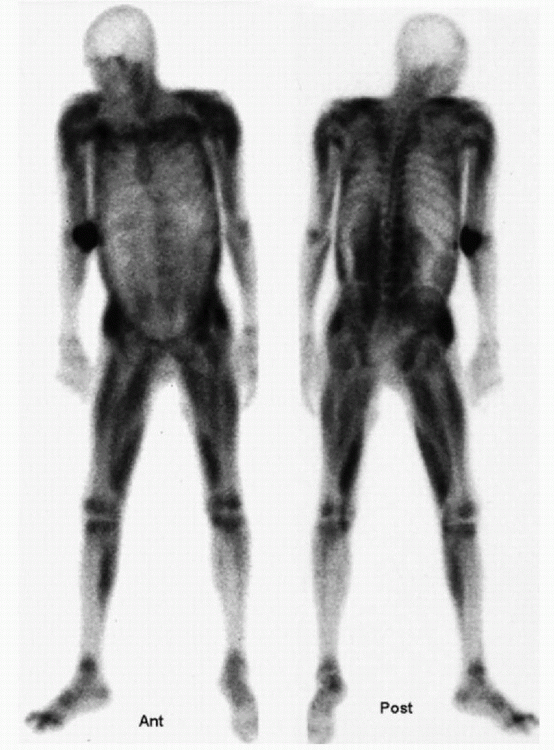
14 A 60-year-old male presents with diffuse bone pain and the following bone scintigraphy? What is the most appropriate next step?
 |
A. Venous duplex sonogram of bilateral lower extremities
B. Radiographs of bilateral lower extremities
C. Computed tomography of the chest
D. MRI of the thoracolumbar spine
E. MRI of bilateral lower extremities
View Answer
14 Answer C. The delayed whole-body bone scintigraphy demonstrates distinct parallel lines of increased cortical/periosteal uptake in bilateral lower extremities (tibiae and femora). The findings are most compatible with hypertrophic osteoarthropathy. It is most commonly seen with lung cancer. As such, correlation with computed tomography of the chest or chest x-ray should be considered to evaluate for a possible malignancy. Other causes of hypertrophic osteoarthropathy include chest infections, COPD, inflammatory bowel disease, liver disease, and congestive heart failure. Shin splints are usually confined to tibiae and often involve only the posteromedial diaphyseal region. The knee radiograph in this patient demonstrated characteristic thick wavy periosteal reaction in the distal femur (arrowheads). Chest CT was recommended based on the bone scintigraphy findings, which demonstrated a left upper lobe mass (arrows). The changes seen on bone scintigraphy often resolve after the treatment of the underlying disease.
 |
References: Uchisako H, Suga K, Tanaka N, et al. Bone scintigraphy in growth hormone-secreting pulmonary cancer and hypertrophic osteoarthropathy. J Nucl Med 1995;36(5):822-825.
Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:301, 308.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:109.
15 Which of the following studies or combination of studies is most appropriate in the evaluation of a suspected hip joint replacement infection?
A. Three-phase bone scintigraphy
B. Labeled leukocyte imaging alone
C. Three-phase bone scintigraphy and sulfur colloid marrow imaging
D. Labeled leukocyte and sulfur colloid marrow imaging
E. F-18 FDG-PET/CT
View Answer
15 Answer D. Radionuclide imaging is currently the imaging method of choice for evaluation of suspected joint replacement infection, and combined labeled leukocyte-marrow imaging is the radionuclide study of choice. It has an accuracy of about 90% for diagnosing prosthetic joint infection. In contrast, according to a meta-analysis by Kwee et al., FDG PET has pooled sensitivity of 87% and specificity of 82% for diagnosing lower extremity prosthetic joint infection.
Both WBCs and sulfur colloid accumulate in bone marrow regardless of location. On the other hand, WBCs accumulate in infection but sulfur colloid does not. As such, when there is incongruent increase in periprosthetic leukocyte accumulation without corresponding increase in marrow activity on colloid imaging, the study is positive for infection. When there is congruent increase in activity on leukocyte and colloid imaging, the findings likely represent marrow expansion/compaction and infection is unlikely.
References: Kwee TC, Kwee RM, Alavi A. FDG-PET for diagnosing prosthetic joint infection: systematic review and metaanalysis. Eur J Nucl Med Mol Imaging 2008;35(11):2122-2132.
Love C, Marwin SE, Palestro CJ. Nuclear medicine and the infected joint replacement. Semin Nucl Med 2009;39(1):66-78.
16 The following patient presents with fatigue, bone pain, hypoalbuminemia, and renal insufficiency. What is the most likely diagnosis?
 |
A. Free pertechnetate
B. Metastatic calcification
C. Hypertrophic osteoarthropathy
D. Metastatic lung cancer
E. Nephrogenic systemic fibrosis
View Answer
16 Answer B. Delayed anterior and posterior whole-body images demonstrate increased radiopharmaceutical uptake in the periarticular regions. There is soft tissue radiopharmaceutical uptake within the thyroid, lungs, stomach, liver, and kidneys. These findings are most compatible with metastatic calcification. Relative photopenia about the left knee is secondary to arthroplasty. Metastatic calcification is calcium deposition caused by abnormal calcium and phosphate metabolism. Increased serum calcium phosphonate product is believed to result in the soft tissue uptake. Thyroid, lungs, heart, stomach, kidneys, and liver are common sites of involvement. It is typically seen in patients with severe hypercalcemia resulting from chronic renal disease, parathyroid tumor, malignancy (i.e., multiple myeloma), and hypervitaminosis D. While free technetium would demonstrate radiopharmaceutical uptake within thyroid and stomach, it would not be present in the lungs or liver. The findings seen are not typical for hypertrophic osteoarthropathy, metastatic lung cancer, or nephrogenic systemic fibrosis.
References: Imanishi Y, Kishiro M, Miyazaki O, et al. Multiple metastatic calcifications detected by bone scintigraphy and demonstrated by CT. Clin Nucl Med 1992;17(2):114-118.
Reitz MD, Vasinrapee P, Mishkin FS. Myocardial, pulmonary, and gastric uptake of technetium-99m MDP in a patient with multiple myeloma and hypercalcemia. Clin Nucl Med 1986;11(10):730.
17 Which of the following statements is MOST accurate regarding the measurement of bone mineral density (BMD) using dual x-ray absorptiometry (DEXA) scan?
A. T-score represents the standard deviation by which the patient’s BMD differs from the mean BMD of a healthy population of the same age, gender, and ethnicity.
B. Z-score represents the standard deviation by which the patient’s BMD differs from the mean BMD of young adult reference population of the same gender and ethnicity.
C. The hip (including total hip and proximal femur) is not a reliable site for measurement in children.
D. When spine or hips cannot be evaluated, the distal one-third (33% radius) of the dominant forearm is the region of choice in the assessment of osteoporosis.
E. Femoral neck is the most reproducible measurement of the hip.
View Answer
17 Answer C. T-score represents the standard deviation by which the patient’s BMD differs from the mean BMD of a young adult reference population of the same sex and ethnicity.
Z-score represents the standard deviation by which the BMD differs from the mean BMD of a healthy population of the same sex, ethnicity, and age as the person undergoing DEXA.
The posterior-anterior (PA) spine and total body less head (TBLH) are the most accurate and reproducible skeletal sites for performing BMD in children. The hip (including total hip and proximal femur) is not a reliable site for measurement in growing children due to the fact that there is a significant variability in femoral maturation, which results in lack of reproducibility in the hip region.
Vertebral bodies are regarded as the optimal site for monitoring response to treatment. However, when vertebral body BMD is compromised, total hip BMD should be used for comparison as it is the most reproducible measurement of the hip.
BMD of the forearm is acquired in the following three scenarios: when two regions from the hip and spine cannot be measured, for patients with hyperparathyroidism, and for patients whose weight exceeds the limit for the table. According to the International Society for Clinical Dosimetry, the distal one-third (33% radius) of the nondominant forearm is the region of choice in the assessment of osteoporosis.
References: Baim S, Binkley N, Bilezikian JP, et al. Official Positions of the International Society for Clinical Densitometry and executive summary of the 2007 ISCD Position Development Conference. J Clin Densitom 2008;11(1):75-91.
Baim S, Leonard MB, Bianchi ML, et al. Official Positions of the International Society for Clinical Densitometry and executive summary of the 2007 ISCD Pediatric Position Development Conference. J Clin Densitom 2008;11(1):6-21.
Kanis JA, on behalf of the World Health Organization Scientific Group (2007, 2008). Assessment of osteoporosis at the primary health-care level (WHO Collaborating Centre, UK) Technical Report. University of Sheffield.
18 The following 3-hour delayed images were acquired after intravenous administration of Tc-99m MDP. Which of the following is most likely associated with this patient?
 |
A. End-stage renal disease with exposure to gadolinium-based contrast agents
B. Elevated creatine phosphokinase levels and renal failure
C. Wrong radiopharmaceutical administration
D. Markedly elevated serum calcium levels
View Answer
18 Answer B. The anterior and posterior whole-body images demonstrate intense uptake of radiopharmaceutical within the musculature as well as relatively reduced renal uptake. Mild radiopharmaceutical uptake is visualized within osseous skeleton suggesting that the correct radiopharmaceutical was injected. These findings are most compatible with severe rhabdomyolysis. Calcium deposition in damaged myocytes is thought to result in radionuclide deposition when combined with phosphate. In rhabdomyolysis, the amount of radiopharmaceutical uptake within the musculature is proportional to the extent of muscle injury. Bone scintigraphy is invariably positive during the acute phase with the greatest uptake occurring in the first 24 to 48 hours, which gradually resolves over a week. As such, it provides a good way of estimating the extent of involvement and allows for following recovery. Patients with rhabdomyolysis typically present with myoglobinuria, elevated creatine phosphokinase levels, and renal failure. Patients with nephrogenic systemic fibrosis (end-stage renal disease with exposure to gadolinium-based contrast agents) would demonstrate more heterogeneous muscular uptake accompanied by increased radiopharmaceutical uptake in the skin and superficial soft tissues, which is not seen in this patient. Metastatic calcifications (markedly elevated calcium levels) would have soft tissue uptake in thyroid, lungs, heart, stomach, liver, and kidneys.
References: Habibian MR. Nuclear medicine imaging: a teaching file, 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2009:395-396.
Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:286, 292, 295.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:121.
19 Which of the following malignancy is LEAST likely to present as a photopenic lesion or “cold” defect on Tc-99m MDP bone scintigraphy?
A. Lymphoma
B. Multiple myeloma
C. Metastatic breast carcinoma
D. Metastatic thyroid carcinoma
E. Metastatic renal cell carcinoma
View Answer
19 Answer C. Since purely lytic lesions do not demonstrate any increase in bony turnover, they may present as photopenic lesions or “cold” defects on bone scintigraphy. As such, sensitivity of bone scintigraphy to detect these lesions is poor. Lesions with purely lytic osseous involvement include multiple myeloma, metastatic renal cell carcinoma, and metastatic thyroid carcinoma. Marrow involvement by lymphoma may also result in the “cold” defects. Of the supplied options, breast cancer is the least likely malignancy to present as a photopenic defect on bone scintigraphy. While statistically, cold bone metastases are most often due to breast carcinoma, they are commonly accompanied by blastic lesions. FDG PET is more sensitive in detecting the lytic lesions, while bone scintigraphy is more sensitive in detecting the blastic lesions. Nonmalignant causes of “cold” lesions include infarction (sickle cell anemia) and avascular necrosis. Changes associated with radiation therapy would result in decreased radiotracer uptake in multiple adjacent bones. This is secondary to a combination of microvascular injury resulting in decreased delivery of the radiotracer, injury to the osteoclast/osteoblast resulting in decreased bony turnover, and fatty replacement of the bone marrow.
References: Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:280.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:99, 104, 106.
20 What is the most likely diagnosis in this patient with the following bone scintigraphic and CT findings?
 |
A. Rhabdomyolysis
B. Myositis ossificans
C. Tibial stress fracture
D. Parosteal osteosarcoma
E. Periosteal osteosarcoma
View Answer
20 Answer B. The anterior, posterior, and left lateral delayed scintigraphic images of the tibia and fibula demonstrate a moderate-sized, oval focus of mild to moderate activity along the anterolateral aspect of the tibia. On CT scan, there is an oval region of ossification within the musculature of the anterolateral shin with mature peripheral calcifications, characteristic of myositis ossificans.
Myositis ossificans, more correctly known as heterotopic ossification, is development of bone in soft tissues such as muscle, tendon, ligaments, or subcutaneous fat. Majority of the cases of focal myositis ossificans/heterotopic bone formation are secondary to direct trauma. Other causes include joint replacement, spinal cord injury, and burn. Postsurgical heterotopic bone formation is commonly visualized around the hip joint. In acute stages, three-phase bone scintigraphy of heterotopic ossification demonstrates hyperperfusion, increased blood pool, and increased uptake on delayed images. As the lesion matures, the degree of radiotracer uptake decreases. Heterotopic ossification is differentiated from bone-forming malignancies such as parosteal or periosteal osteosarcoma by the presence of more mature calcifications along the periphery rather than in the center. With osteosarcoma, the bone formation would be more organized and dense centrally and less organized and dense along the outer edge.
References: Habibian MR. Nuclear medicine imaging: a teaching file, 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2009:397-398.
Mettler FA, Guiberteau MJ. Essentials of nuclear medicine imaging, 6th ed. Philadelphia, PA: Saunders, 2012:286, 292, 295.
Ziessman HA, O’Malley JP, Thrall JH. Nuclear medicine: the requisites, 4th ed. Philadelphia, PA: Saunders, 2014:121.
21 A 36-year-old lady undergoes whole-body bone scintigraphy secondary to diffuse bone pain. Based on the findings, what is the most appropriate next step?
 |
A. Chest radiograph
B. Mammogram
C. Lumbar spine radiographs
D. DEXA scan
E. Serum parathyroid hormone level
View Answer




21 Answer B. Delayed anterior and posterior whole-body scintigraphy images demonstrate asymmetrically increased radiopharmaceutical uptake within an enlarged right breast (arrowheads). The findings are highly suspicious for primary breast malignancy. As such, further correlation with mammography should be considered. Increased activity within the left axilla (black arrow) is likely secondary to combination of physiologic breast uptake and overlap of radiopharmaceutical uptake within the soft tissues. A subsequent contrast-enhanced CT of this patient demonstrated presence of a large necrotic mass within the right breast (asterisk). The contour abnormality of the bladder seen on the anterior images was secondary to enlarged uterus from leiomyomata (#). Differential considerations of increased breast activity on bone scintigraphy include mastitis and trauma.
Related posts:
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
